Acid/Base And Electrolytes
- Hyponatremia
- Hypernatremia
- Hypokalemia
- Hyperkalemia
- Hypomagnesemia
- Hypermagnesemia
- Hypocalcemia
- Hypercalcemia
- Hypophosphatemia
- Hyperphosphatemia
- Algorithm For Acid Base Disorders
- Assessment Of RTAs
Hyponatremia
Definition
- Mild: Serum Na 130-134mmol/L
- Moderate: Serum Na 120-129mmol/L
- Severe: Serum Na <120mmol/L
- Acute: <48hrs since development of hyponatremia
- Chronic: >48hrs since development of hyponatremia. (hyponatremia should be considered chronic whenever the duration is unknown.
Evaluation: Order serum osmolality, urine sodium, urine osmolality, TSH, Lipid panel.
Tips: Free water balance (Urine osmolality) is regulated by ADH. Sodium excretion (urine sodium) is regulated by aldosterone. If a patient has ESRD, the cause of hyponatremia is excess free water intake in the setting of impaired Kidney water excretion, and is not mediated by ADH.
Step 1: Differentiate from true hyponatremia from pseudohyponatremia.
- A normal or elevated effective serum osmolality (280mOsm/kg or greater) suggests pseudohyponatremia.
- Hypertonic states, like hyperglycemia or mannitol use, can cause hyponatermia by drawing water extracellularly and lowering serum sodium concentration. This is a true hyponatremia. Serum osmolality will be high, sodium should normalize with correction of hypertonic state.
- Correction formula for hyperglycemia: corrected Na = measured Na + [(serum glucose - 100)/100] x 1.6 . You can also use MD Calc
- Hyperlipidemia or increased protein can also cause a lab error that results in a falsely low sodium result.
Step 2: is ADH high or low? Compare serum osmolality to urine osmolality.
- If serum osm > urine osm, then ADH is low (kidneys are appropriately responding by maximizing water excretion). Causes are excess water intake or inadequate solute intake. A urine osm <100 also suggests normal free water excretion.
- If serum osm < urine osm, ADH is high. Proceed to step 3
- Check for iatrogenesis: are there high rates of hypotonic solution infusing?
- Look at what medications are mixed in (ex: IV abx in 500ml D5W 4x/day = 2L of free water).
- Check volume of free water flushes in patients getting tube feeds or other hypotonic oral intake.
- Consider primary polydipsia.
- Causes of inadequate solute intake: tea and toast diet (carbs and fats metabolize to water and CO2, so do not count as solutes), beer potomania (high beer intake relative to solute intake).
Step 3: If ADH is high, what is the volume status?
If ADH is activated, urine osmolality is usually >100. Urine Na can help to determine RAAS activation, which can narrow the differential in casese where volume status is not clear. A low urine Na (<20) suggests RAAS activation, as seen in hyper or hypovolemia; a high urine sodium may suggest SIADH.
Hypervolemic: DDx: CHF, nephrotic syndrome, liver failure.
- ADH is released in response to low effective arterial blood volume due to third spacing or poor perfusion.
- Urine Na will be low (<20) since the RAAS is activated in response to low arterial blood flow.
Hypovolemic:
- ADH is being released in response to low effective arterial blood flow due to fluid loss
- Extrarenal losses, like GI loss: urine Na will be low (<20) since aldosterone will also be activated
- Renal salt wasting: urine Na will be high (>20). Causes include salt-wasting nephropathy, adrenal insufficiency, cisplatin, thiazide diuretic use.
Euvolemic:
- Hypothyroidism: check TSH (The main mechanism for the development of hyponatremia in patients with chronic hypothyroidism is the decreased capacity of free water excretion due to elevated antidiuretic hormone levels)
- Glucocorticoid deficiency: check AM cortisol
- SIADH: Inappropriate release of ADH independent of effective arterial blood flow. Urine Na will be high, since aldosterone is low.
- SIADH is a diagnosis of exclusion with following features:
- Clinical euvolemia
- Normal thyroid and adrenal function, no recent diuretic use
- Lab findings: Urine osmolality >150mOsm, serum osm <275 mOsm, Urine Na >20 mmol/L with normal dietary salt intake.
Management: Repeat BMP q4hr. Goal to increase Na no more than 4 to 6 mEq/L in 24hrs to prevent osmotic demylination syndrome. Start treatment based on volume status
Evaluate and treat severe symptoms emergently in all patients
-
The presence of these signs suggests cerebral edema and required rapid treatments: visual changes, neurologic deficits, encephalopathy, coma, respiratory arrest, and seizures.
-
Start on hypertonic 3% saline immediately at rate 15 to 30mL/hr and consult nephrology. Monitor serum sodium hourly while on hypertonic saline. If sodium is correcting too fast, stop hypertonic saline and start on D5W infusion.
Select treatment approach based on volume status, severity, and etiology.
Hypovolemia:
- Start on IV fluids Normal saline @100mL/hr. Caution: once volume status is corrected, a brisk aquaresis may ensue and cause overcorrection, thus, strict urine output and frequent sodium monitoring is critical. The earliest and most concerning indication of overcorrection is brisk urine output and/or a decrease in urine osmolality.
SIADH:
- Treatment of underlying cause/withdrawal of causative agents as possible.
- Start with fluid restriction 1-1.5L/day but restriction alone is often inadequate. Do not restrict beyond 1L, as that is unlikely to add additional benefit and can cause significant discomfort.
- Use urine electrolytes (Urine sodium + Urine potassium) to guide therapy:
- UNa + UK < serum Na: Positive free water clearance. Patient is still urinating out free water but not enough to improve hyponatremia. This suggests fluid restriction will be an effective treatment.
- UNa + UK > serum Na: Negative free water clearance. All free water is reabsorbed and any urination will continue to lower serum Na. This suggests osmole supplementation (hypertonic saline or salt tabs) is needed to treat hyponatremia.
- Any IV fluids with Na content less than UNa + UK will result in worsening hyponatremia because the kidney is able to excrete the solute but reabsorb the free water from the infused solution. Therefore, UNa + UK >154 is typically an indication that hypertonic saline is needed to correct hyponatremia.
- Additional therapies for SIADH:
- Hypertonic saline: Effective (3% = 513mEq/L), necessary when UNa+UK is very high. Requires good venous access. Not a long term therapy.
- NaCl tabs: 1g NaCl tab = 17mEq Na and 17 mEq Cl. Not a very high osm load per tab (typically need upwards of 2g TID). Difficulty pill burden, can stimulate thirst counteracting fluid restriction and cause GI upset.
Hypervolemia:
- Free water restriction (1-1.5L.day)
- Loop diuretics to optimize volume status
- Hypertonic saline and salt tabs generally NOT recommended as they will worsen volume overload.
If the serum sodium has been overcorrected:
- IV D5W
- Can give 3mL/kg/hr D5W to lower [Na] by approximately 1mEq/L/hr if overcorrected
- Pay attention to ongoing losses: if urine output is brisk (>150mL/hr) and dilute, the patient is losing free water rapidly and it is raising serum Na rapidly. Suggest nephro consultation to assist with safe correction strategies (eg: titrating D5W drip to a % of urine output or using DDAVP to inhibit the aquaresis)
Diagnosis and Management of disorders of body tonicity-Hyponatermia and Hypernatremia
Clinical practice guideline on diagnosis and treatment of hyponatremia
Hypernatremia
Definition:
- Serum Na >135 mmol/L. Chronic means > 48 hours. Acute means < 48hrs.
Etiology:
Renal water loss (U osm <700-800)
- loop diuretics
- Osmotic diuresis (hyperglycemia, mannitol, urea)
- Diabetes Insipidus: Central (trauma/post-surgical, pituitary lesions, sheehan's syndrome) vs Nephrogenic (congenital, sickle cell, hypercalcemia, severe hypokalemia, drugs: lithium, amphotericin)
Extra-renal water loss (U osm >700-800)
- GI loss: vomiting, NGT, osmotic diarrhea, lactulose, malabsoption
- Insensible loss: fever, burns, exercise
- hypertonic intake: hypertonic saline, excess salt intake, hypertonic sodium bicarb pushes
Evaluation: U osm, U Na, volume status
- Causes is often apparent from history and review of medications, nutrition, and intake/output
- Determine if there is inappropriate renal free water loss
- In DI, urine will be inappropriately dilute (<300 mOsm/L). Water deprivation test will result in rising serum Na and persistently dilute urine. Desmopression response after deprivation can differentiate nephrogenic (no response) vs central (concentrated urine)
Management
Step 1: calculate free water deficit. Can also use MD Calc

- % body water for 0.6 for male and 0.5 for female. If elderly use 0.5 for male and 0.45 for female
- Give free water deficit enterally
- Do not forget to correct Na if hyperglycemia also present

Step 2: Rate of correction
- Divide free water deficit by 24hrs and give accordingly. Check serum Na every 6-12hrs to adjust correction rate and follow urine output
- Rate of correction depends on acuity of onset and risk:
- chronic (>48hrs): 12 mEq/d appears safe w/o risk of cerebral edema
- acute (<48hrs): may decrease Na by 2 mEq/L/h until Na 145
- hyperacute (min-hrs) & life threatening (ICH, seizure): rapidly infuse D5W plus minus emergent HD
Diagnosis and Management of Disorders of Body Tonicity-Hyponatremia and Hypernatremia
Rate of correcting of hypernatremia
Hypokalemia
Definition:
- Serum <3.5mmol/L
Etiology:
- Intracellular shifts: Hypothermia, Exogenous insulin/refeeding, beta-agonists
- GI Potassium loss
- Metabolic acidosis: diarrhea, laxative abuse
- Metabolic alkalosis: Vomiting, NGT
- Renal Potassium Losses
- Hypotensive or normotensive
- Metabolic Acidosis: DKA, RTA type I and II
- Metabolic Alkalosis: diuretic (thiazide > loop)
- Drugs: amphotericin, cisplastin
- Hypomagnesemia
- Hypertensive: Mineralcorticoid excess
- Hypotensive or normotensive
Evaluation:
Review medication list
Order basic labs: Serum BMP, Mg, Serum osmolality, urine electrolytes (Na, K, Cl), Urine osmolality
Distinguish renal from GI losses with urine potassium.
- Urine K/Cr >13 mEq: Renal loss ; Urine K/Cr <13mEq: extrarenal loss
- If inappropriately high urine potassium excretion, consider sending plasma renin activity and aldosterone level
- High renin: suggests diuretics, GI losses, renovascular disease
- Low renin and high aldosterone: primary aldosteronism
- Low renin and low aldosterone: non-aldosterone mineralcorticoid excess such as licorice ingestion
Severe hypokalemia, get an EKG. Changes include U wave, inverted T wave, ST depression, PR and QRS prolongation and can lead to Vfib.
Management: There is a replacement protocol that can be ordered. So the RN can replaced it based on the hospital protocol.
- Replete magnesium first if low
- Replete potassium to >3 or >4 if high risk (HTN, CHF, arrythymia, MI, cirrhosis)
- Supplementation can be given Oral or IV. Oral potassium replacement is first choice. Caution in patient with peptic ulcer disease. Higher doses can cause stomach upset.
- Suggested potassium replacement doses.
- Serum K: 3.7-3.8: 20 mEq KCl IV or PO
- Serum K: 3.5-3.6: 40 mEq KCl IV or PO
- Serum K: 3.3-3.4: 60 mEq KCl IV or PO
- Serum K: 3.1-3.2: 80 mEq KCl IV or PO
- Serum K: less than equal 3.0: 100mEq KCl IV or PO
Caution in renal failure or ESRD. Always check the creatinine prior to replacing potassium. Give about half the suggested dose of potassium in patient with decreased GFR
Disorders of potassium homeostasis. Hypokalemia and hyperkalemia
Hyperkalemia
Definition
- Serum K+ >5.3-5.5
Etiology:
- Pseudohyperkalemia- K release from cells after blood draw, IVF with K
- Impaired excretion
- Low GFR (AKI or CKD)
- Drugs (spironolactone, ACEi, ARB, TMP-SMX, NSAIDs, digitalis overdose, heparin, chemo therapeutic agents)
- Shift from intracellular to extracellular compartment
- Excessive K intake
- Hemolysis
- Marked thrombocytosis or leukocytosis
- Ingestion (K Supplements, dietary salt substitutes)
- Iatrogenic
- Low mineralocorticoid state (adrenal insufficiency, type IV RTA)
- Acidosis
- Insulin deficiency or resistance including DKA
- Cell death (rhabdomyolysis, burns, tumor lysis)
- Retroperitoneal hemorrhage
- Old (hemolyzed) pRBC transfusion
Clinical manifestations:
- Weakness, nausea, paresthesia, palpitations
Evaluation:
- Repeat serum K+ and assess renal function studies including serum Cr and BUN
- Order stat ECG to evaluate for hyperkalemia related changes (Tall peaked “tented” T waves, PR interval prolongation followed by loss of P waves, QRS widening, sinus wave pattern, VF/asystole/PEA
- Review medications for offending drugs and stop as appropriate/indicated
Management: PowerChart “Hyperkalemia (TH) Protocol”
Approach to Rx:
-
Order ECG for serum K >5.5 and treat emergently if ECG changes noted. Rx any K >6.5 emergently regardless of ECG changes
-
Repeat ECG every 30-60 mins to ensure resolution of ECG abnormalities and consider telemetry for monitoring.
-
Check and treat concurrent electrolyte abnormalities as they increase risk for arrythmias
-
Check if sample is hemolyzed and repeat serum K measurement to verify
Treatment aims:
- Stabilize the myocardial membrane
- Temporarily shift K into cells
- Eliminate K from body
Cardiac membrane stabilization:
- Calcium chloride 0.5-1g IV (more potent, but must be given via central line)
- Calcium gluconate 1-2g IV
- No effect on serum K level. Should normalize ECG. If not, re-dose.
Temporarily shift K into cells:
- Regular Insulin 10 units IV + D50 100ml IV. If high risk for hypoglycemia, monitor blood glucose closely. If hyperglycemic, insulin can be given alone.
- Beta2-agonists (albuterol 10-20mg in 4mL saline nebulized)
- NaHCO3 50-100 mEq
Eliminate K from body:
- Preferably renal elimination
- IVF with NS or NaHCO3- First line in hypovolemic patients
- Loop diuretic: Furosemide 40-160 mg IV- First line in hypervolemic patients and given with IVF if euvolemic
- Thiazide diuretic: Adjunct use with loop diuretic may be useful
- GI cation exchangers- Exchange Na+ for K+ in the GI tract
- Sodium zirconium cyclosilicate (Lokelma)- 10 g TiD for up to 48hr, then 5-15g q.other daily-daily as maintenance
- Kayexalate (sodium polystyrene sulfonate)- 15-30 g PO (slow onset and controversial use; associated with bowel necrosis and contraindicated in post-op patients and those with risk of/obstruction
- Dialysis-can be used in patients with acute/chronic renal failure who fail medical management; improves serum K relatively quickly but lengthy process to initiate therapy (nephrology consult, machine and catheter placement)
- Continues renal replacement therapy-slow correction and requires ICU setting
Key Points:
-
Hyperkalemia protocol can be initiated/ordered from PowerChart
-
Serum K level >6.5 or hyperkalemia with ECG changes warrant emergent treatment with calcium gluconate or CaCl
-
Strategy to shift K into cells is useful acutely as it works fast but is only a temporary measure and it should be accompanied by therapies to eliminate K from the body
-
K elimination renally is most efficient and takes into consideration patient’s volume status
Hypomagnesemia
- Serum Mg++ <1.8 mg/dL
Etiology:
- Malnutrition (assc. with heavy chronic alcohol use causing renal wasting)
- Malabsorption or diarrhea/GI loss
- PPI induced
- Renal losses (polyuria and high tubular flow, e.g., osmotic diuresis, post-ATN diuresis)
- Hypercalcemia (e.g. hyperparathyroidism)
- Loop and thiazide diuretic associated
- Proximal tubular toxins (e.g. aminoglycosides, amphotericin, cisplatin)
- Calcineurin inhibitors (tacrolimus > cyclosporine)
- Volume expansion (reduced Mg++ reabsorption due to reduced Na and H2O reabsorption)
- Gitleman and Bartter syndromes
- Uncontrolled DM, post-parathyroidectomy (Hungry bone syndrome)
Clinical manifestations:
- NM hyperexcitability (tremor, tetany, convulsions), weakness, delirium, coma
- CV (widening QRS, peaked T waves, wide PR interval, atrial and ventricular arrhythmias)
- Hypocalcemia, hypoparathyroidism, PTH resistance, and decreased calcitriol synthesis
Evaluation:
- Order CMP, serum Mg++ and Phosphorus level
- Review patient history, clinical circumstances, nutritional status and medications
Management: PowerChart “Electrolyte Replacement Protocol”
Approach to Rx:
Route and dose based on severity of clinical manifestations and degree of hypomagnesemia
Patients with no or minimal symptoms:
- PO repletion recommended if able to tolerate
- Can give IV if unable or have GI side effects (discomfort, diarrhea)
- Typical daily PO dose in patients with normal renal function is 240-1000mg (20-40 mEq of elemental Mg++ in divided doses
Patients with severe symptoms: tetany, arrhythmias, seizure
- 1-2 grams (8-16 mEq) Magnesium sulfate bolus over 2-15mins if hemodynamically unstable (including those with arrhythmias consistent with torsade de pointes or hypomagnesemic hypokalemia). Repeat bolus if remains hemodynamically unstable
- If hemodynamically stable, give 1-2 grams Magnesium sulfate in 50-100mL of D5W over 5-60mins followed by infusion of 4-8 grams MgSulfate slowly over 12-24 hrs
- Adjust dose in AKI and CKD due to risk for severe hypermagnesemia
- Measure serum Mg 6-12 hrs after each IV dose and adjust dose accordingly
For routine IV or maintenance repletion, use the following estimated repletion doses:
- If the plasma Mg++ is < 1 mg/dL, give 4 to 8 grams (32 to 64 mEq of magnesium sulfate over 12 to 24 hours and repeat as needed.
- If the plasma Mg++ is 1 to 1.5 mg/dL, give 2 to 4 grams (16 to 32 mEq of magnesium sulfate over 4 to 12 hours.
- If the plasma Mg++ is 1.6 to 1.9 mg/dL, give 1 to 2 grams (8 to 16 mEq of magnesium sulfate over 1 to 2 hours.
(Conversion relationships: 1 mmol = 2 mEq = 24 mg of elemental magnesium = 240 mg magnesium sulfate.)
Key Points:
- Correct the underlying disease
- Correct Mg++ based on severity of hypomagnesemia and symptoms if any
- Great caution should be exercised when treating hypomagnesemia in AKI and CKD patients due to the increased risk for severe hypermagnesemia
- Replacement therapy with IV magnesium in patients with arrhythmias or NM symptoms
Hypermagnesemia
Definition
- Serum Mg++ >2.3 mg/dL
Etiology:
- Insufficient excretion due to CKD
- Iatrogenic/excess intake due to overaggressive replacement, Magnesium-based laxatives/enemas use in CKD, Mg++ administration during preeclampsia/eclampsia treatment
Clinical manifestations:
Symptoms are either cardiovascular vs neuromuscular manifestations or hypocalcemia
- Plasma Mg++8-7.2mg/dL: Nausea, flushing, headache, lethargy, drowsiness and hyporeflexia
- Plasma Mg++2-12mg/dL: Somnolence, hypocalcemia, areflexia, hypotension, bradycardia and ECG changes
- Plasma Mg++ >12: Muscle paralysis leading to flaccid quadriplegia, apnea/respiratory failure, complete heart block, cardiac arrest
Evaluation:
- Order CMP, serum Mg++
- Review patient history, clinical circumstances and medications
Management:
Treatment is tailored based on severity and clinical manifestations and renal function
- Asymptomatic patients: Cessation of Mg++ supplementation therapies
- Symptomatic patients: 1gram Calcium Gluconate IV over 10mins to antagonize Mg++
- Moderate renal impairment (eGFR 15-45): Consider IV Isotonic fluid plus loop diuretic (e.g., Furosemide)
- Severe renal impairment (eGFR <15)/Symptomatic patients: Dialysis is the definitive therapy
Key Points:
- Clinically relevant hypermagnesemia is rare and is usually due to excessive magnesium administration in patients with CKD or impaired magnesium excretion
- Severe hypermagnesemia may need dialysis
Hypocalcemia
Evaluation:
- verify with repeat measurement that there is a true decrease in the serum calcium concentration (total serum calcium corrected for albumin or ionized calcium)
- Note alkalosis augments calcium binding to albumin and increases severity of symptoms
- Compare with previous values if available
- If the patient has a low albumin-corrected serum calcium or ionized calcium concentration, further evaluation to identify the cause is indicated
- Obtain thorough history and physical examination.
- measure serum intact parathyroid hormone (PTH)
- Other measurements that may be helpful include serum magnesium, creatinine, phosphate, vitamin D metabolites (primarily 25-hydroxyvitamin D [25(OH)D]), and alkaline phosphatase.
Causes:
- renal failure
- hypoparathyroidism or pseudohypoparathyroidism (PTH resistance)
- severe hypomagnesemia or hypermagnesemia
- acute pancreatitis
- rhabdomyolysis
- tumor lysis syndrome
- vitamin D deficiency
Signs:
- paresthesias, tetany (especially carpopedal spasm), lethargy, confusion, seizures,
Trousseau's sign, Chvostek's sign, decreased cardiac function, QT prolongation
Treatment:
- Symptomatic hypocalcemia ( see symptoms above) or asymptomatic hypocalcemia with an acute decrease in serum corrected calcium to ≤7.5 mg/dL (≤1.9 mmol/L) or ionized calcium to ≤3 mg/dL (≤0.8 mmol/L) should be corrected by replacement with calcium gluconate IV.
- 1 or 2 g of calcium gluconate, equivalent to 90 or 180 mg elemental calcium, in 50 mL of 5% dextrose or normal saline) can be infused over 10 to 20 minutes
- If present, low Mg should also be corrected because it contributes to low Ca.
For those with milder symptoms of neuromuscular irritability (paresthesias) and corrected serum calcium concentrations greater than 7.5 mg/dL (1.9 mmol/L) or a serum ionized calcium concentration greater than 3.0 mg/dL (0.8 mmol/L), initial treatment with oral calcium supplementation is sufficient. If symptoms do not improve with oral supplementation, IV calcium infusion is required.
Hypercalcemia
Evaluation:
- verify with repeat measurement that there is a true increase in the serum calcium concentration (total calcium corrected for albumin or ionized calcium)
- Compare with previous values if available
- Clinical evaluation, including duration of hypercalcemia, presence or absence of symptoms, family history, and medications, may help determine the etiology of hypercalcemia
Causes:
- primary hyperparathyroidism
- malignancy (PTH related peptide, ectopic production of 1,25, dihydroxyvitamin D, osteoclast activating factor
- lytic bone mets
- non parathyroid endocrine disorder
- thyrotoxicosis, pheochromocytoma, adrenal insufficiency, VIP-producing tumor
- granulomatous disease (1,25 dihydroxyvitamin D excess)
- sarcoidosis, tuberculosis, histoplasmosis, coccidiomycosis, leprosy
- medications (thiazide diuretics, lithium, estrogens, antiestrogens)
- milk-alkali syndrome
- vitamin A or D intoxication
- familial hypocalciuric hypercalcemia
- immobilization
- parenteral nutrition
- acute and chronic renal failure
Signs:
- "Stones, moans, groans, with psychic overtones*.
- Renal: polyuria (nephrogenic DI), nephrolithiasis, renal failure, ectopic calcification
- Gl: anorexia, nausea, vomiting, constipation
- Neuro: weakness, fatigue, confusion, stupor, coma
- ECG: Shortened QT
Treatment:
- avoid factors that can aggravate hypercalcemia, including thiazide diuretics and lithium carbonate therapy, volume depletion, prolonged bed rest or inactivity, calcium and/or vitamin D supplements, and a high-calcium diet (>1000 mg/day)
- Mild hypercalcemia - asymptomatic or mildly symptomatic with with serum calcium level of 12 and 14 mg/dL [3 to 3.5 mmol/L]) may not require immediate therapy
- Moderate hypercalcemia - Asymptomatic or mildly symptomatic individuals with chronic moderate hypercalcemia (calcium between 12 and 14 mg/dL [3 to 3.5 mmol/L]) may not require immediate therapy
- Severe hypercalcemia - serum calcium levels of >14 mg/dL [3.5 mmol/L]) or symptomatic (eg, lethargy, stupor) require aggressive therapy.
- → Initial therapy of severe hypercalcemia includes the simultaneous administration of intravenous (IV) isotonic saline, subcutaneous calcitonin, and a bisphosphonate (typically, IV zoledronic acid)
- Correct dehydration, increase renal calcium excretion, decrease bone resorption, and treat the underlying disorder.
- IV hydration, initial rate is 200 to 300 mL/hour that is then adjusted to maintain the urine output at 100 to 150 mL/hour
- In individuals with renal insufficiency or heart failure, careful monitoring and judicious use of loop diuretics (after intravascular volume has been repleted) may be required to prevent fluid overload. IV furosemide
- Specific treatment in approximate desirability of use:
- For immediate, short-term management in severe hypercalcemia (Ca >14 mg/dl) and symptomatic patients (lethargy, stupor), administer Calcitonin in combination with NS hydration and Bisphosphonates. Initial Calcitonin dose is 4 units/kg, administered SQ or IM. Repeat serum calcium in 4-6 hrs. If lowering of calcium levels is noted, continue 4 U/kg BID for 24-48 hrs. May increase to 8 U/kg Q12H or Q6H for 24-48 hrs if response is not satisfactory with 4 U/kg BID.
- Among IV bisphosphonates, Zaldronic Acidis preferred over pamidronate (60 to 90 mg over 2 hours) because it is superior to pamidronate in reversing hypercalcemia related to malignancy. The initial dose is 4 mg IV over 15 minutes.
- Pamidronate 15-45 mg IV as single IV infusion or 90 mg over 2-24 hours would be another option for treatment
https://www.uptodate.com/contents/treatment-of-hypercalcemia?search=hypercalcemia&source=search_result&selectedTitle=2~150&usage_type=default&display_rank=2
Hypophosphatemia
Evaluation:
- Serum phosphorus levels should be interpreted with concomitant evaluations of PTH, serum total and ionized calcium, urine phosphate and calcium and Vitamin D
- Medical history, physical examination and lab tests to determine etiology of hypophosphatemia (renal wasting, decreased intestinal absorption etc)
- Concomitant serum levels of Magnesium and Potassium should be checked as well and replaced per protocol
Causes:
- Hyperparathyroidism
- Vitamin D deficiency
- Malabsorption/emesis
- Increased urinary secretion
- Refeeding after malnutrition
- Hyperalimentation
- Recovery of DKA, effects of insulin/glucagon/androgens
- Hypothermia (recovering from hypothermia)
- Steatorrhea
- Medication (e.g. phosphate binders, salicylate poisoning, steroids, diuretics)
- Decreased intake
- Alcohol abuse, withdrawal
- Renal tubular defects (aldosteronism, SIADH)
- Sepsis
- Gout
- Burns
- Respiratory alkalosis
- Hypomagnesemia
Signs: Generally seen with serum phosphate levels below 1 mg/dl
- Numbness
- Weakness
- AMS / confusion
- stupor
- Seizures
- coma
- Muscle pain
- Rhabdomyolysis
- Resp. failure
- CHF
- Paresthesias
- Dysarthria
- Hemolysis
- Platelet dysfunction
- Metabolic acidosis
Therapy:
- Treat underlying cause, the phos levels will normalize automatically ( DKA, diarrhea, chronic antacid therapy, or vitamin D deficiency)
- Replete if serum phos levels are less than 2.0 mg/dl (0.64 mmol/L)
- Keep phos levels over 1 mg/dl, above that, oral replacement is preferable to avoid hyperphosphatemia ( which can cause subsequent hypocalcemia, ectopic calcifications, renal failure, or hypotension)
- In Asymptomatic patients with serum levels below 2.0 mg/dl replete with oral phosphate
- Serum level of 1.5 mg/dl (0.48 mmol/L) → give 1 mmol/kg elemental phosphorus (minimum of 40 and maximum of 80 mmol can be given in 4 doses over 24h)
- Serum level less than 1.5 mg/dl → give 1.3 to 1.4 mmol/kg of elemental phosphorus (up to a maximum of 100 mmol given in 4 doses over 24h)
- In Symptomatic patients treatment varies with severity of the hypophosphatemia
- Serum level of 1.0 to 1.9 mg/dl (0.32 to 0.63 mmol/L) → treat with oral phosphate
- Serum level less than 1.0 mg/dl → treat with IV phosphate and switch to oral
- Stop replacement when serum levels is equal to or greater than 2.0 mg/dl
- IV preparations: IV phosphate is potentially dangerous. If IV phos is necessary, use dose depending on severity of hypophosphatemia and the weight of the patient.
- If the serum phosphate concentration is greater than or equal to 1.25 (0.40 mmol/L), → give 0.08 to 0.24 mmol/kg over six hours (up to a maximum total dose of 30 mmol).
- If the serum phosphate concentration is less than 1.25 mg/dL (0.40 mmol/L) → give 0.25 to 0.50 mmol/kg over 8 to 12 hours (up to a maximum total dose of 80 mmol).
→ measure serum phosphate levels Q6H and switch the oral replacement once serum levels have reached 1.5 mg/dl (0.48 mmol/L)
- Use either sodium phosphate or potassium phosphate depending on whether patient also needs potassium
- Follow Potassium and Magnesium as well and replete per protocol
https://www.uptodate.com/contents/hypophosphatemia-evaluation-and-treatment?search=hypophosphatemia&source=search_result&selectedTitle=1~150&usage_type=default&display_rank=1#H727383
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4324571/#:~:text=When%20evaluating%20a%20patient%20with,not%20reliable%20indicators%20of%20total
Hyperphosphatemia
Definition
- Serum Phosphate >4.5mg/dL.
Etiology/Risk Factors
- Increased intake (external/internal):
- Excessive vitamin D (increases GI absorption of PO4) or vitamin A.
- Phosphate-containing enema, particularly in patients with kidney insufficiency.
- PO4 replacement.
- TPN (through administration of excess phosphate).
- Excessive dietary phosphate in patients with advanced CKD (usually Stage >4).
- Shifts from cells into serum:
- Acidosis (lactic acidosis, DKA).
- Hypoinsulinemia.
- Rhabdomyolysis.
- Tumor lysis.
- Decreased excretion/increased reabsorption:
- Bisphosphonates.
- Decreased PTH secretion or renal resistance to PTH (hyper- or hypomagnesemia).
- Kidney disease (GFR <30).
- Often accompanied by hypocalcemia due to calcium-phosphorus complex formation.
Evaluation
Laboratory tests to order:
- CMP.
- Calculate a calcium-phosphate product ([Calcium] x [Phosphate]).
- At risk for calciphylaxis, renal osteodystrophy, and ectopic calcification if product > 55.
- LDH, uric acid if clinical concern for tumor lysis syndrome.
- CK if clinical concern for rhabdomyolysis.
Management
- ACUTE: rhabdomyolysis, tumor lysis, exogenous phosphate load.
- If acute process and developing renal failure or symptomatic (with severe hypocalcemia), may require hemodialysis.
- If kidney function is preserved, most causes of hyperphosphatemia will resolve by addressing the underlying cause (stopping vitamin D, resolution of tumor lysis, etc.). IV fluids may be given to facilitate phosphate excretion.
- CHRONIC: chronic kidney disease and secondary hyperparathyroidism.
- Low phosphate diet and phosphate binders as necessary (sevelamer, calcium acetate, lanthanum carbonate, etc.). Dialysis removes phosphorus, but given that only a small fraction of phosphorus is in plasma, there is significant rebound post-HD, hence the need for adjunctive therapies.
Key Points
- If kidney function is preserved, most other causes of hyperphosphatemia will resolve by addressing the underlying cause.
- Consider hemodialysis for acute, severe hyperphosphatemia complicated by symptomatic hypocalcemia and AKI/CKD.
- Hemodialysis (3x/week) is not typically effective for chronic hyperphosphatemia, and most patients with ESRD will require low phosphate diet and phosphate binder therapy.
- Calculate calcium-phosphate product to determine risk for complications.
Algorithm For Acid Base Disorders
Before You Begin: Gather Data
What lab tests do you need?
- ABG vs. VBG
- VBG can provide reliable estimation for pH (0.02-0.04 lower than ABG) and HCO3 (1-2 mEq higher than ABG).
- pCO2 on VBG is higher than arterial PaO2 by 4-9mmHg.
- ABG is necessary to accurately assess PaCO2 in hypercapnia or severe shock.
- BMP.
- Albumin.
Step 1: Determine Primary Acid-Base Disturbance.
- Remember that chronic acid-base disturbance(s) and/or mixed acute acid-base disturbances can be obscured by a normal pH.
- Consider the following “normal” values:
• Arterial pH: 7.40
• Arterial pCO2: 40
• Bicarb (HCO3): 24
• Anion gap: 12 - Acidemia
• pH < 7.38
• Primary disturbance
• Respiratory acidosis = pCO2 > 42
• Metabolic acidosis = HCO3 < 22 - Alkalemia
• pH > 7.42
• Primary disturbance
• Respiratory alkalosis = pCO2 < 38
• Metabolic alkalosis = HCO3 > 26
Step 2a: Calculate and Interpret the Anion Gap
- Anion gap (AG) = [Na] – [Cl] – [HCO3].
- Normal AG = 8-12 mEq/L with a serum albumin of 4g/dl.
- The normal AG depends on serum albumin. The expected "normal" range for AG can be calculated by 2.5 x albumin (g/dl) +/- 2.
- For severe hypoalbuminemia (2.0 g/dl), the expected gap would be 5 +/- 2, and an AG of 8-12 would be abnormally elevated.
- Paraproteinemia (especially polyclonal or monoclonal IgG) can lower anion gap due to the abundance of cations added to the system; this should be accounted for when evaluating anion gap since it could obscure a truly elevated AG.
- For calculation, >12 is generally used as the cutoff for a high AG. Because 12 is the upper limit of normal, keep in mind that approach might increase specificity for elevated AG at the cost of sensitivity. Because of person-to-person variation in “normal” AG, it can be useful to review a patient’s previous values of AG to establish a baseline and give context to small, acute changes in AG.
- If the AG is elevated, there is an anion gap metabolic acidosis present. Proceed to step 2b.
- If the AG not elevated, there is not an anion gap metabolic acidosis present. Proceed to step 3.
Step 2b: Calculate and Interpret the Excess Anion Gap
- If there is an anion gap, determine whether the excess in AG fully explains the drop in bicarbonate.
- For every 1 unit increase in AG (△AG↑) from its upper limit of normal value (12), there is an expected 1 drop in HCO3 (△HCO3↓) from its “normal” value (24).
- If the AG and HCO3 are balanced, (△HCO3 ± 5mmol/L ≈ △AG), there is no concurrent metabolic process.
- If the HCO3 is lower than expected (△HCO3 ± 5mmol/L > △AG), there is a concurrent non-elevated anion gap metabolic acidosis as evidenced by a reduction of HCO3.
- If the HCO3 is higher than expected (△HCO3 ± 5mmol/L < △AG), there is a concurrent metabolic alkalosis as evidenced by an excess of HCO3.
- The 5mmol/L correction accounts for the normal range of bicarbonate.
- Alternate approach to answer this question: “correcting” the bicarb.
- Corrected HCO3 = HCO3 + (AG - 12).
- If the sum is greater than the usual bicarbonate range (> 28), there is a concomitant metabolic alkalosis. If the sum is less than the usual bicarbonate range (< 22), there is a concomitant non-elevated anion gap metabolic acidosis.
- Finally, there is a third approach to this same problem, “the delta-delta,” which is not discussed here.
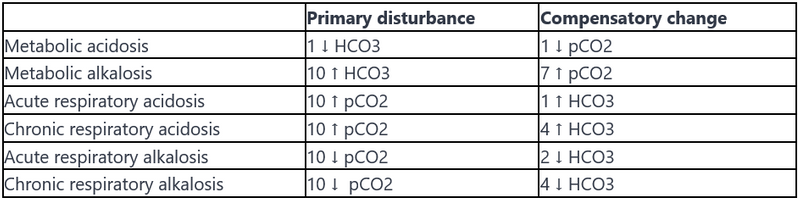
Step 3: Evaluate for Compensation
Evaluate for physiologic compensation for the acid-base disorder.
Any values above or below expected suggest an additional acid-base disturbance; a compensation should not normalize or overcorrect the pH.
The following table gives a quick rule-of-thumb for evaluating compensation. More detailed formulas are listed below.
Common Questions in Metabolic Acidosis
-
What is the pathophysiology of saline-induced normal anion gap (hyperchloremic) metabolic acidosis?The normal anion gap metabolic acidosis resulting from large volume administration of normal saline (NS) can be explained as a dilutional effect on the existing bicarbonate level. This is because NS contains a supraphysiologic concentration of chloride (154 mEq/L) and no bicarbonate; thus it will raise serum chloride while diluting other anions - namely lowering bicarbonate - inducing a metabolic acidosis. This may be avoided by using a balanced intravenous solution such as Lactated Ringer’s or Plasmalyte. These solutions have a lower [Cl-] concentration compared to NS and, most importantly, contain lactate and acetate respectively, which are rapidly metabolized to an equimolar amount of bicarbonate.
-
What are the disadvantages of giving bicarbonate in the setting of acute metabolic acidosis?
-
Can cause an initial transient worsening of intracellular acidosis.
-
Can lead to generation of increased CO2 which causes respiratory acidosis (especially in patients with respiratory failure such as in ARDS).
-
Can represent a large sodium load that can exacerbate hypervolemia.
-
Can worsen hypokalemia.
-
-
The 2008 Surviving Sepsis guidelines recommend against its use in sepsis if pH > 7.15. One can consider temporary NaHCO3 administration in the setting of severe metabolic acidosis (pH < 7.1) or to facilitate permissive hypercarbia. In most cases of normal anion gap metabolic acidosis, it is probably safe. Consider renal replacement therapy in cases of severe acidosis refractory to medical therapy.
Key Points
- It is important to follow a systematic approach each time interpreting a blood gas. Establish the primary disorder. Calculate AG to reveal an anion gap metabolic acidosis (can be hidden when pH is normal but mixed disorders are present). Compare △AG and △HCO3 to look for concurrent metabolic alkalosis or normal anion gap metabolic acidosis. Use a compensation chart/formula to reveal “overcompensation” or “undercompensation” which indicates the presence of another disorder.
- The presence of a normal pH with abnormal pCO2 and bicarbonate suggests a mixed acid-base disorder with counterbalancing acidosis and alkalosis.
- The pCO2 and serum bicarbonate typically move in parallel with an isolated acid-base disorder; both are high OR both are low. For example, a respiratory acidosis will have an increased pCO2 with a compensatory increase in serum bicarbonate. If the pCO2 and serum bicarbonate move in opposite directions (one high and one low), then you should consider the possibility of two simultaneous primary acid-base disorders (i.e., a mixed acid-base disorder).
- A mixed acid-based disorder consists of any combination of at least two disorders: two metabolic disturbances OR one respiratory and one metabolic. Triple acid-base disorders include one respiratory disorder (acidosis or alkalosis) with two metabolic disorders (high gap and normal gap metabolic acidosis OR high gap metabolic acidosis and metabolic alkalosis).
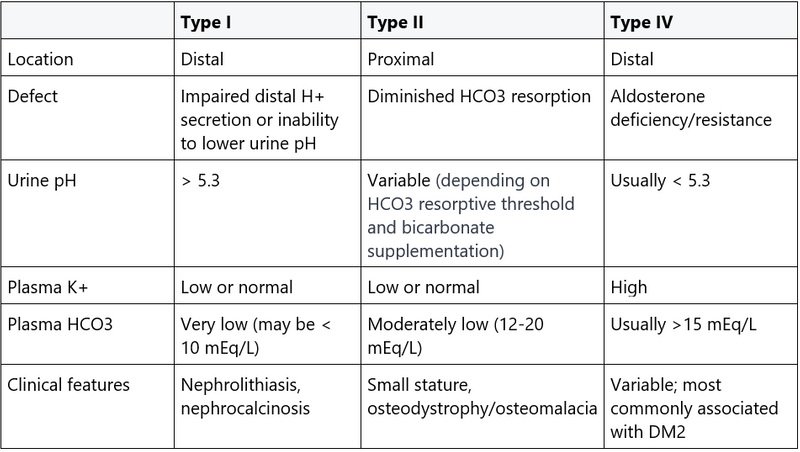
Assessment Of RTAs
Definition
- Renal tubular acidosis refers to an impaired acid-base metabolism by the kidney in the setting of normal glomerular filtration. These conditions are characterized by a non-elevated anion gap (hyperchloremic) metabolic acidosis.
- Kidney disease must be excluded as etiology of inappropriate acid-base metabolism.
- Chronic kidney disease (CKD) is associated with a non-elevated anion gap acidosis early in its course due to decreased generation of NH3 and decreased medullary trapping of NH4+.
- As CKD progresses, elevated anion gap acidosis tends to predominate as the kidney loses the ability to excrete anions (phosphate, sulfate, urate, etc.).
- Note: in the setting of acidemia, the expected urine pH is between 4.5-5.0 as virtually no HCO3 should be excreted.
Categories
- Type I RTA (distal)
-
- Etiology: Type I RTA represents a failure to secrete H+ in the distal nephron, where urinary acidification takes place. This leads to metabolic acidosis with higher than appropriate urine pH, as the body is unable to acidify the urine to eliminate systemic acid.
- Causes
- Most common: in adult patients, urinary obstruction or Sjogren’s/SLE
- Primary (genetic)
- RA
- Myeloma
- Marked volume depletion
- Drugs
- Cyclosporine toxicity
- Amphotericin
- TMP/SMX can impair Na channels leading to a functional type I RTA. - Features/diagnosis
- Serum HCO3 may be <10 mEq/L as there is no way to excrete the acid load and bicarbonate is depleted by buffering the excess serum acid.
- Urine pH > 5.5, reflecting defect in urinary acidification. If a small amount H+ is secreted, it will be buffered by NH3.
-
- Type II RTA (proximal)
-
- Etiology: Type II RTA represents a failure to reabsorb filtered bicarbonate in the proximal tubule, causing substantial HCO3 wasting. Normally, reclamation of 80-90% of filtered HCO3 occurs in the proximal tubule; the distal nephron only absorbs a modest amount of bicarbonate.
- Causes
- Most common: for adult patients, multiple myeloma or nucleotide analogues (e.g., tenofovir), which causes a proximal tubule injury that manifests as Fanconi syndrome.
- Primary (genetic)
- Acetazolamide
- Heavy metals (Pb, Cd, Hg, Cu, others)
- Inherited and acquired Fanconi syndrome: generalized proximal tubular dysfunction with impaired ability to reabsorb one or more substrates that normally should be reabsorbed (e.g., bicarbonate, potassium, low molecular weight protein, glucose). It may be caused by any of the above etiologies. - Features/Diagnosis
- Serum HCO3 levels are usually maintained between 12-20 mEq/L. The serum HCO3 level approximates the tubule’s absorptive capacity: as the serum HCO3 level drops, the filtered load of HCO3 into the proximal tubule will decrease to the point that it can be fully reabsorbed.
- Urine pH can be variable, depending on the level of serum HCO3. Bicarbonate administration may affect the urine pH, as described below.
- If enough HCO3 is given, it may raise serum HCO3 level enough to overwhelm the reabsorptive capacity of the proximal tubule. This leads to HCO3 loss (spillover) in the urine, raising urine pH > 5.5.
- If serum HCO3 remains low, all of the filtered HCO3 can be reabsorbed, and there will be less HCO3 in the urine. Urine pH will be <5.3 due to normal H+ secretion by the functioning distal nephron.
- Look for accompanying electrolyte abnormalities in type II RTA, like hypokalemia, hypophosphatemia, and glucosuria.
-
- Type IV RTA- most common type of RTA in adults.
-
- Etiology: In Type IV RTA, aldosterone deficiency or resistance in the intercalated and principal cells of the distal nephron leads to hyperkalemia and impaired NH3/NH4+ production, thus causing metabolic acidosis.
- Causes
- Hypoaldosteronism-mediated
- Diabetic nephropathy (most common cause).
- Chronic interstitial nephropathy.
- Drugs (NSAIDS, heparin, ACEI/ARB, trimethoprim, calcineurin inhibitors).
- Addison's disease.
- Aldosterone-resistance mediated
- Sickle cell anemia (most common cause of aldosterone resistance).
- Urinary tract obstruction.
- Features/diagnosis
- Serum HCO3 usually > 15 mEq/L.
- Urine pH < 5.3. In contrast to type I RTA, there is insufficient NH3 production in type IV RTA, leaving the few H+ produced to be left unbuffered, thus leading to a lower urinary pH.
-
Evaluation
- Serum: ABG and CMP.
- Urine: UA/urine culture (UTI from urea-producing organisms can raise urine pH by metabolism of HCO3 and NH4+), urine lytes (Na, K, Cl).
- Can also use expanded urine lytes to calculate urinary osmolar gap (Na, Cl, K, BUN, glucose, osmolality); see discussion below.
- Serum potassium
- Hypokalemia: type II RTA (proximal) or type I RTA (distal).
- Hyperkalemic: type IV RTA (hypoaldosteronism) or type I RTA (distal). - Calculate urine anion gap (UAG):
- UAG is a surrogate for urine NH4+, the unmeasured cation in the urine.
- UAG = UNa + UK – UCl.
- UAG < 0 suggests extrarenal cause of normal anion gap metabolic acidosis. The kidney is appropriately compensating for the acidosis by secreting NH4+.
- UAG > 0 suggests renal cause (UAG may be negative in some cases of proximal RTA).
- UAG should not be used if there is excretion of another anion (lactate, DKA anions, etc.) OR if urine sodium <20 mEq/L (insufficient Na+ delivery to distal tubule does now allow for H+ exchange required for urinary acidification). - If urine sodium <20 mEq/L, consider calculating urine osmolal gap (UOG) instead.
- UOG = 2(UNa +UK) + Uurea/2.8 + Uglucose/18.
- UOG <50 is suggestive of RTA.
Treatment
- Type I and II: aggressive K supplementation followed by HCO3 supplementation (initial HCO3 supplementation can worsen hypokalemia, especially in proximal RTA).
- Use NaHCO3 or Na-citrate to replete.
- Bicarbonate goals
- Type I: normal serum HCO3.
- Type II: HCO3 >20 mEq/L. - Note: may also need close monitoring/repletion of calcium and phosphate.
- Type IV: treat hyperkalemia.
- Restrict dietary potassium, avoid potassium-sparing diuretics.
- Use loop diuretics and thiazides for potassium excretion.
- Can consider fludrocortisone in severe cases (recommend nephrology consultation before initiating).
Key Points