Gastroenterology
GI bleed
Etiology
- The site of bleeding is only suggested by the patient’s presentation and physical examination.
- Stool can turn black (melena) with as little as 50-100 cc of upper GI bleeding
Pre-endoscopic clinical risk stratification
Clinical judgment always comes first.
- Assess the following features, based in part upon Rockall scale, BLEED criteria and Glasgow-Blatchford score.
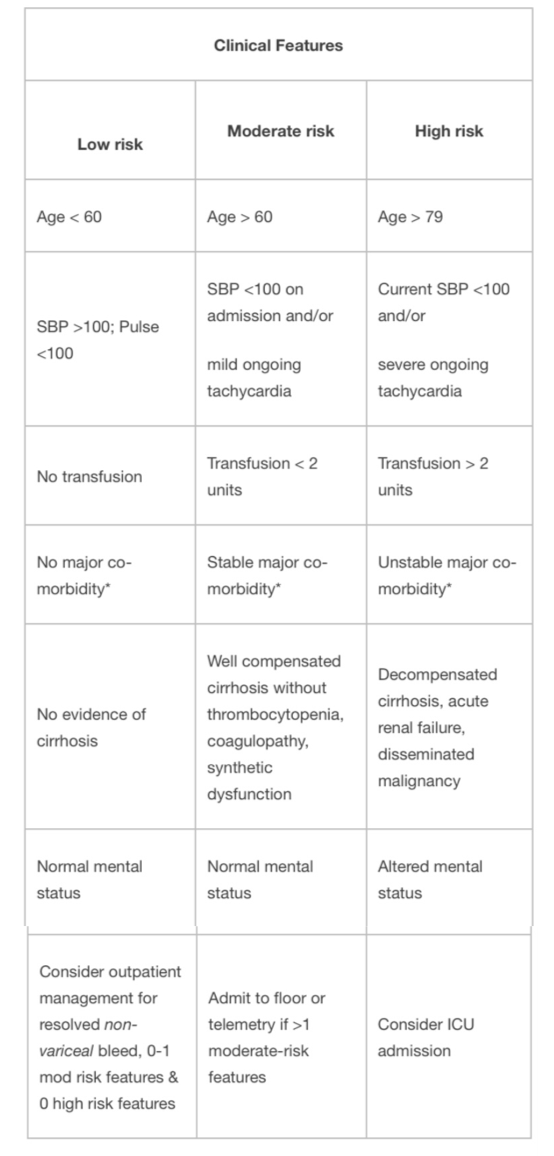
*Major co-morbidity defined as CAD, CHF, renal failure, liver disease, sepsis, disseminated malignancy, altered
mental status, pneumonia, COPD, asthma.
- Use clinical risk to determine urgency of endoscopy and level of care required.
- Absolute indications for ICU admission:
- Shock
- Orthostasis
- Acute HCT decrease by >6%
- Transfusion requirements >2units pRBCs
- Active bleeding – ongoing hematemesis, bright red blood per NGT, hematochezia
- Most deaths are secondary to respiratory, cardiovascular, infectious, and renal complications associated with bleeding, not from exsanguination.
Evaluation
- Risk factors/Hx: NSAID use, alcohol use, liver disease/varices, severe retching, h/o GI bleed, past endoscopy, prior abdominal surgery, aortic aneurysms/grafts, trauma, coagulopathy, anticoagulation, malignancy
- Physical Exam:
- VS (with orthostatics)
- Rectal – note the color/consistency of stool (black/tarry = melena; bright red blood = hematochezia), palpable masses, external anal findings (e.g., hemorrhoids, fissures), smear stool on paper towel to see true color/content
- Guaiac testing is not useful to determine inpatient management
- Abdominal mass, peritoneal signs
- Stigmata of ESLD (asterixis, ascites, spiders, palmar erythema, caput, jaundice, testicular atrophy, gynecomastia)
- HEENT: epistaxis, telangiectasias (hereditary hemorrhagic telangiectasias, EtOH.)
- NG lavage is not required for upper GI bleeding patients. Endoscopist may use in certain patients to triage the timing of endoscopy but should not be placed routinely. It can be helpful in severe hematochezia patients to differentiate brisk upper GI bleed from lower GI bleeding.
- Coagulopathy and varices are not contraindications to NG tube placement.
- Note amount of aspirate obtained, the quality of the aspirate, and amount of saline lavage that is required to clear it.
- The lack of blood in the NG aspirate does not rule out an upper GI bleed as it may have only sampled gastric content and bleed may be duodenal
- Bile in the aspirate may confirm placement beyond the pylorus
- Low threshold to get KUB if peritoneal signs or abdominal distension. CT is more sensitive for free air, perforation, or ischemia.
- ECG for patients with a history of CAD or age > 45.
Management
Evaluation and Stabilization:
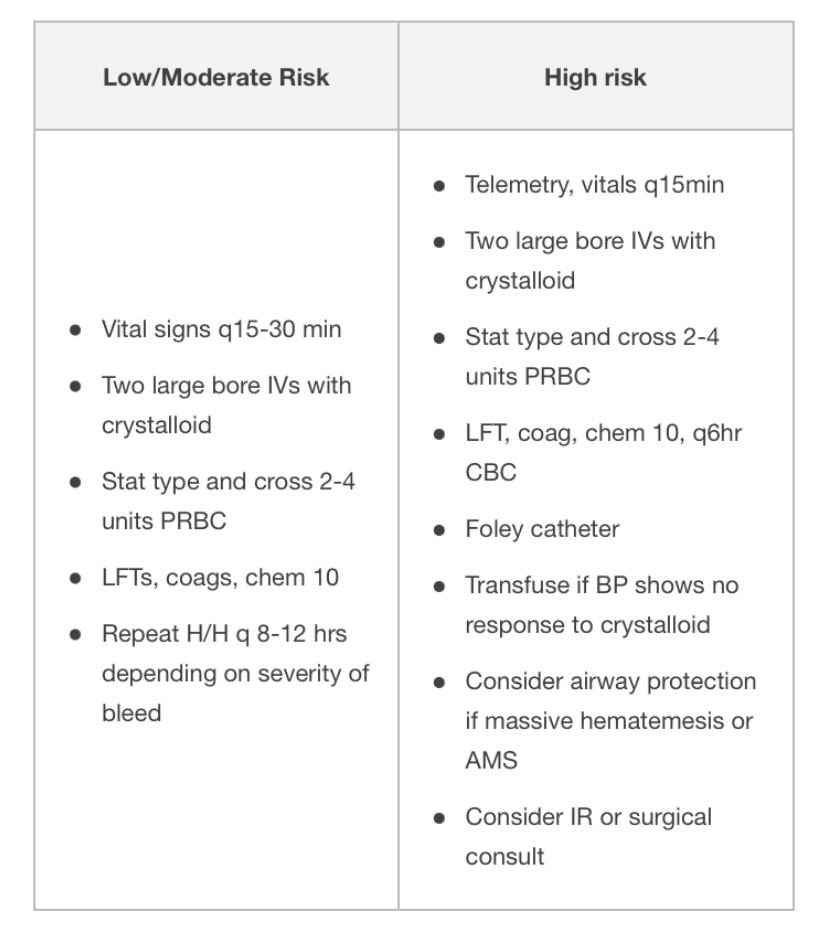
Common Management of Upper and Lower GI bleed
- NPO until cleared by GI
- Volume resuscitate with crystalloid.
- 2 large bore (16g or larger) PIVs.
- Consider cordis or rapid infusion catheter instead of triple lumen for central access.
- Most recent studies support restrictive transfusion strategies (goal Hg>7), though may consider goal of Hg>8 for patients with CAD.
- Protonix (bolus 80mg IV x 1 à 8mg/hr IV gtt)
- Reduces mortality in lesions subsequently seen to have high-risk stigmata for rebleed, reduces rebleeding after endoscopy, length of stay, and need for transfusion in patients with high-risk ulcer
- PPI before endoscopy: no difference in mortality, re-bleed rate, or need for surgery than if given after endoscopy, but decreases rate of high-risk stigmata of re-bleeding and need for subsequent endoscopic therapy
- Check H. pylori (serologies, endoscopic biopsy, stool antigen) and treat if present.
- H. Pylori diagnostic testing has higher false-negative rates in setting of bleeding (or PPI use.) Repeat if negative in setting of acute bleeding and clinical suspicion is high.
- Consider FFP, vitamin K if INR > 1.5, prothrombin complex concentrate (such as Kcentra), DDAVP (0.3 mcg/kg IV q12h x 2 doses) if uremic bleeding, and platelets if platelet count < 50. In ESLD patients, also order fibrinogen & replete with cryoprecipitate to >100.
- Consider massive transfusion protocol if hemodynamically unstable/requiring large amount of blood products.
- Complications of massive transfusion:
- metabolic alkalosis (2/2 citrate metabolism) in setting of renal impairment
- hypokalemia (precipitated by alkalosis)
- hypocalcemia (due to citrate binding)
- hypothermia
- hyperkalemia (particularly with older blood products)
- Avoid NSAIDs, ASA, anticoagulants
- Surgery consult if recent surgical procedure or rebleeding (>6u pRBC)
- Re-bleeding:
- Preferred treatment is repeat endoscopic therapy
- If patient has persistent bleeding after endoscopy, consider CT angiogram or IR embolization. For uncontrolled bleeding requiring >6u pRBC there is no significant difference (rates of re-bleeding, subsequent therapy, or mortality) for IR embolization vs. surgical intervention.
- Other diagnostic modalities (discuss with GI first)
- Tagged RBC scan (can detect bleed rate >0.1cc/min, localizes bleeding to area of abdomen but variable localization to portion of intestinal tract, can re-scan several times over 24-48h after tagged RBC administration for intermittent bleeding). If positive, consider IR embolization.
- CT (mesenteric) angiography (requires >1 cc/min.)
Specific management for suspected variceal bleed
- Goal hemoglobin > 7, plt >50, INR <1.5. More aggressive resuscitation may result in higher rates of re-bleed due to increase in portal pressures, particularly if Hb > 9.
- Octreotide 100 mcg bolus then 50 mcg/hr x 72 hours (constrict splanchnic circulation.)
- Discontinue PPI drip after endoscopy if there is no ulcer.
- Ceftriaxone (1gm q24 hrs x 5 days): reduces variceal re-bleeding, infection, and mortality in patients with cirrhosis +/- ascites.
- Endoscopy fails to control bleeding in ~10-20% patients.
- For persistent bleeding or re-bleed:
- Repeat endoscopic therapy
- Balloon tamponade (e.g. Sengstaken-Blakemore,tube): 50% rate of re-bleed upon balloon deflation, other complications including esophageal necrosis, rupture.
- TIPS
- Surgery
- Beta blockers: use in patients with proven variceal bleeds after the acute bleed has resolved and s/p octreotide x 72 hours. Nonspecific beta blockers (propranolol, nadolol) can be used as secondary prophylaxis against variceal re-bleeding .
- Titrate to a dose that lowers the baseline heart rate by 25% or to goal heart rate 55-60, as tolerated by the patient (15-30% of patients won’t tolerate due to low blood pressure.)
- Arrange for GI follow-up (endoscopy) for serial banding.
Endoscopy
- Diagnostic and therapeutic, as well as prognostic
- Correction of anticoagulation should not delay endoscopy
The following are endoscopic findings that a GI consultant uses to further risk stratify patients:
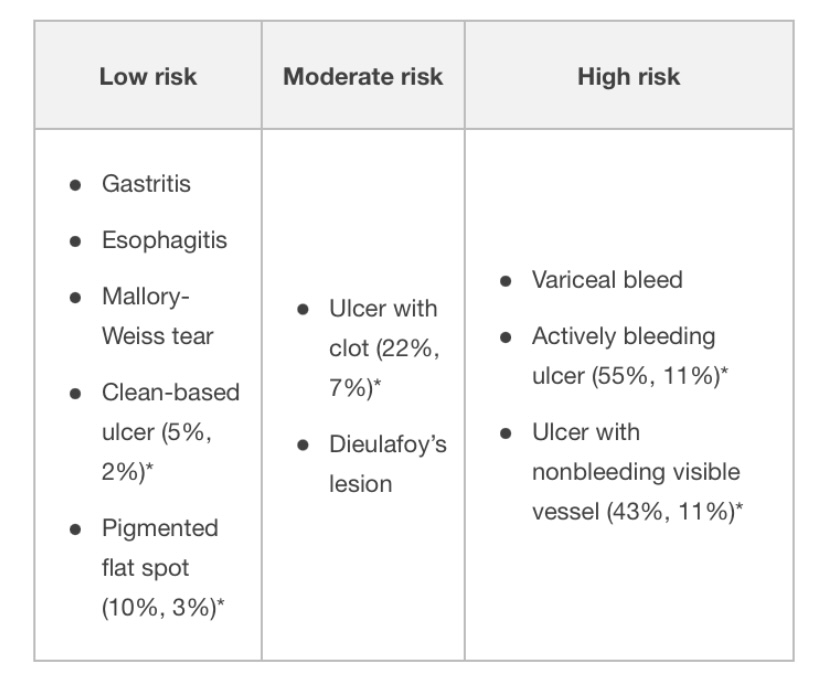
* Risk of (rebleeding, mortality rate)
- Length of observation for re-bleeding after endoscopy depends on endoscopic and clinical risk criteria. Rapid post-endoscopy discharge is reasonable for some patients with low-risk endoscopic findings, but discuss with GI first.
Key points
- Melena requires as little as 50-100 cc of blood and usually signals upper GI bleed, but can occur with light colonic bleeding with a slow transit time
- Most deaths occur from respiratory, cardiovascular, infectious, and renal complications associated with bleeding, and not exsanguination.
- NG tube lavage is not routinely required in all GI bleed patients
- The lack of blood in the NG aspirate does not rule out an upper GI bleed
Reference: Hospitalist Handook
Ascites
Definition
- Accumulation of peritoneal fluid
Symptoms
- Abdominal Distention and discomfort
- Anorexia
- Nausea
- Early satiety
- Heartburn (Gastroesophageal Reflux)
- Flank Pain
- Respiratory distress
Signs
- Umbilicus may evert
- Bulging flanks with the patient lying supine
- Fluid Wave Test
- Shifting Dullness Test
- Puddle Sign
Most common etiologies
- Cirrhosis (Cirrhotic Ascites): 85% of cases
- Cancer (Malignant Ascites)
- Congestive Heart Failure
- Tuberculosis
Labs
- Diagnostic abdominal Paracentesis
- Ascites Fluid: Cell Count with Differential, albumin/protein concentration and ascitic fluid inoculation in blood culture bottles, Serum Ascites albumin gradient (SAAG), cytology
Ascites fluid assorted labs
Serum
- CBC, CMP (electrolyte imbalance, LFT, hepatorenal), BNP, PT, aPTT, INR,
Imaging
Medication Management
- Spironolactone and
- Thiazide or Loop Diuretic (diuretic dosage should be adjusted to a daily weight loss of no more than 500 g/day in patients without peripheral edema and 1 kg/day in patients with peripheral edema)
- Electrolyte correction
- Consider Hepatic encephalopathy management
- Paracentesis (consider Albumin)
- Antibiotic (therapeutic/prophylaxis for SBP)
- Electrolyte replacement, restriction of daily sodium intake to 80–120 mmol
Executive summary of recommendations
-
Diagnostic paracentesis in new- onset ascites
-
1.1. A diagnostic paracentesis is recommended in all patients with new-onset ascites. (Quality of evidence: moderate; Recommendation: strong)
-
1.2. The initial ascitic fluid analysis should include total protein concentration and calculation of the serum ascites albumin gradient (SAAG). (Quality of evidence: moderate; Recommendation: strong)
-
1.3. Ascites fluid analysis for cytology, amylase, brain natriuretic peptide (BNP), and adenosine deaminase should be considered based on the pretest probability of specific diagnosis (Quality of evidence: moderate; Recommendation: weak)
-
-
Spontaneous bacterial peritonitis
-
2.1. Diagnostic paracentesis should be carried out without delay to rule out spontaneous bacterial peritonitis SBP) in all cirrhotic patients with ascites on hospital admission. (Quality of evidence: moderate; Recommendation: strong)
-
2.2. A diagnostic paracentesis should be performed in patients with GI bleeding, shock, fever or other signs of systemic inflammation, gastrointestinal symptoms, hepatic encephalopathy, and in patients with worsening liver or renal function. (Quality of evidence: moderate; Recommendation: strong)
-
2.3. Ascitic neutrophil >250/mm3 count remains the gold standard for the diagnosis of SBP and this can be performed either by manual microscopy or using automated counts, based on flow cytometry for counting and differentiating cells. (Quality of evidence: moderate; Recommendation: strong)
-
2.4. Ascitic fluid culture with bedside inoculation of blood culture bottles should be performed to guide the choice of antibiotic treatment when SBP is suspected. (Quality of evidence: moderate; Recommendation: strong)
-
2.5. Immediate empirical antibiotic therapy should be determined with due consideration of the context of SBP (community-acquired or healthcare-associated), the severity of the infection, and the local bacterial resistance profile. Cefotaxime has been widely studied, but the choice of antibiotic should be guided by local resistance patterns and protocol. (Quality of evidence: moderate; Recommendation: strong)
-
2.6. A second diagnostic paracentesis at 48 hours from the start of treatment to check the efficacy of antibiotic therapy should be considered in those who have an apparently inadequate response or where secondary bacterial peritonitis is suspected. (Quality of evidence: low; Recommendation: weak)
-
2.7. Patients presenting with gastrointestinal bleeding and underlying ascites due to cirrhosis should receive prophylactic antibiotic treatment (cefotaxime has been widely studied but the antibiotic should be chosen based on local data) to prevent the development of SBP. (Quality of evidence: strong; Recommendation: strong)
-
2.8. Patients who have recovered from an episode of SBP should be considered for treatment with norfloxacin (400 mg once daily), ciprofloxacin (500 mg once daily, orally), or co-trimoxazole (800 mg sulfamethoxazole and 160 mg trimethoprim daily, orally) to prevent a further episode of SBP. (Quality of evidence: low; Recommendation: weak)
-
2.9. Primary prophylaxis should be offered to patients considered at high risk, as defined by an ascitic protein count <1.5 g/dL. However, it is important that the potential risks and benefits and existing uncertainties are communicated to patients. (Quality of evidence: low; Recommendation: weak)
-
-
Dietary salt restriction
-
3.1. Patients with cirrhosis and ascites should have a moderately salt-restricted diet with a daily salt intake of no more than 5–6.5 g (87–113 mmol sodium). This translates to a no added salt diet with avoidance of precooked meals. (Quality of evidence: moderate; Recommendation: strong)
-
3.2. Patients with cirrhosis and ascites should receive nutritional counseling on the sodium content in the diet. (Quality of evidence: weak; Recommendation: strong)
-
-
Diuretics
-
4.1. In patients with the first presentation of moderate ascites, spironolactone monotherapy (starting dose 100 mg, increased to 400 mg) is reasonable. In those with recurrent severe ascites, and if faster diuresis is needed (for example, if the patient is hospitalized), combination therapy with spironolactone (starting dose 100 mg, increased to 400 mg) and furosemide (starting dose 40 mg, increased to 160 mg) is recommended. (Quality of evidence: moderate; Recommendation: strong)
-
4.2. All patients initiating diuretics should be monitored for adverse events. Almost half of those with adverse events require diuretic discontinuation or dose reduction. (Quality of evidence: low; Recommendation: weak)
-
4.3. Hypovolaemic hyponatremia during diuretic therapy should be managed by discontinuation of diuretics and expansion of plasma volume with normal saline. (Quality of evidence: low; Recommendation: weak)
-
4.4. Fluid restriction to 1–1.5 L/day should be reserved for those who are clinically hypervolaemic with severe hyponatremia (serum sodium <125 mmol/L). (Quality of evidence: low; Recommendation: weak)
-
4.5. Hypertonic sodium chloride (3%) administration should be reserved for those who are severely symptomatic with acute hyponatremia. Serum sodium should be slowly corrected. (Quality of evidence: low; Recommendation: weak)
-
4.6. It may be appropriate to consider the use of midodrine in refractory ascites on a case-by-case basis. (Quality of evidence: low; Recommendation: weak)
-
-
Large volume paracentesis (LVP)
-
5.1. Patients should give informed consent for a therapeutic or diagnostic paracentesis. (Quality of evidence: low; Recommendation: strong)
-
5.2. Ultrasound guidance should be considered when available during LVP to reduce the risk of adverse events (Quality of evidence: low; Recommendation: weak)
-
5.3. Routine measurement of the prothrombin time and platelet count before therapeutic or diagnostic paracentesis and infusion of blood products are not recommended. (Quality of evidence: moderate; Recommendation: strong)
-
-
Use of human albumin solution (HAS)
-
6.1. Albumin (as 20% or 25% solution) should be infused after paracentesis of >5 L is completed at a dose of 8 g albumin/L of ascites removed. (Quality of evidence: high; Recommendation: strong)
-
6.2. Albumin (as 20% or 25% solution) can be considered after paracentesis of <5 L at a dose of 8 g albumin/L of ascites removed in patients with ACLF or high risk of post-paracentesis acute kidney injury. (Quality of evidence: low; Recommendation: weak)
-
6.3. In patients with SBP and increased serum creatinine or rising serum creatinine, infusion of 1.5 g albumin/kg within 6 hours of diagnosis, followed by 1 g/kg on day 3, is recommended. (Quality of evidence: low; Recommendation: weak)
-
-
Transjugular intrahepatic portosystemic shunt (TIPSS)
-
7.1. TIPSS should be considered in patients with refractory ascites. (Quality of evidence: high; Recommendation: strong)
-
7.2. Caution is required if considering TIPSS in patients with age >70 years, serum bilirubin >50 µmol/L, platelet count <75×109/L, a model for end-stage liver disease (MELD) score ≥18, current hepatic encephalopathy, active infection or hepatorenal syndrome. (Quality of evidence: moderate; Recommendation: strong)
-
-
Umbilical hernia
-
8.1. Suitability and timing of surgical repair of umbilical hernia should be considered in discussion with the patient and multidisciplinary team involving physicians, surgeons, and anesthetists. (Quality of evidence: low; Recommendation: strong)
-
-
Hepatic hydrothorax (HH)
-
9.1. TIPSS should be considered in patients with HH after discussion with the multidisciplinary team. (Quality of evidence: low; Recommendation: strong)
-
9.2. In patients with HH who are not undergoing a TIPSS and/or a liver transplant evaluation, alternative palliative interventions should be considered. (Quality of evidence: low; Recommendation: strong)
-
-
Non-selective beta-blockers (NSBB) and ascites
-
10.1. Refractory ascites should not be viewed as a contraindication to NSBB. (Quality of evidence: moderate; Recommendation: strong)
-
10.2. Patients with refractory ascites who are taking NSBB should be monitored closely, and dose reduction or discontinuation may be appropriate in those who develop hypotension or acute/progressive renal dysfunction. (Quality of evidence: moderate; Recommendation: strong)
-
Reference
- Pedersen JS, Bendtsen F, Møller S. Management of cirrhotic ascites. Ther Adv Chronic Dis. 2015;6(3):124-137. doi:10.1177/2040622315580069
- , et al Guidelines on the management of ascites in cirrhosis
SBP
Definition
SBP is a bacterial infection of the ascitic fluid.
Diagnosis:
PMN count >= 250 cells/mm3 OR ascitic fluid WBC >= 500 cells/mm3 with a positive fluid culture.
Diagnostic clinical signs: New onset fever, confusion or abdominal pain, hepatic encephalopathy, vomiting, diarrhea.
Diagnosis of Culture-negative neutrocytic ascites: PMN count >= 250 cells/mm3 with a negative fluid culture (subtract 1 PMH for every 250 RBCs).
Pathogens causing SBP: Common organisms are E. coli, Klebsiella pneumoniae, Enterobacteriaceae, Streptococcus pneumoniae, and Enterococcus.
Patients with Cirrhosis: Cirrhotic patients can also get secondary bacterial peritonitis, which usually requires surgical intervention. One should suspect secondary peritonitis with perforation if the ascitic fluid meets 2 or more of the following: Total WBC >10,000, Total protein > 1 g/dl, Glucose < 50 mg/dl OR LDH > 225 milliunits/ml (or higher than upper normal for serum). One should also be suspicious if multiple organisms are cultured or if there is a failure to improve after 48 hours of standard therapy.
Risk Factors for SPB: Severe liver disease, GI hemorrhage, Prior SBP, Ascitic fluid protein <= 1 g/dl.
Diagnosis of SBP: Abdominal paracentesis, send fluid for cell count and differential and send fluid directly in the culture bottles.
Treatment for SBP:
Start antibiotic therapy as soon as the diagnosis of SBP is made based on fluid PMN count OR earlier if clinically indicated.
Use a third-generation cephalosporin (cefotaxime or a similar third generation cephalosporin) HIGH dose 2gm every 8 hours for 5 days.
Any person with cirrhosis and ascites who has signs or symptoms concerning for SBP should be treated with antibiotic therapy regardless of ascites fluid PMN count.
Antibiotic Prophylaxis for SBP: Prophylaxis should be given to persons with cirrhosis with a prior history of SBP or acute GI bleeding and should be considered in those who have renal or hepatic dysfunction if total ascitic fluid protein is less than 1.5g/dL.
Primary and Secondary SBP Prophylaxis: Ciprofloxacin 500 mg daily or trimethoprim-sulfamethoxazole one double strength tablet daily. If patient has cirrhosis and acute GI hemorrhage, IV ceftriaxone 1 gram daily is recommended for a total duration of 7 days.
Acute Pancreatitis
Definition
indicates inflammation of the pancreas.
Acute pancreatitis: results from the leakage of pancreatic enzymes into pancreatic tissue, leading to autodigestion.
Chronic pancreatitis: causes are varied and lead to destruction of the pancreatic tissue. Patients may present with pain and/or weight loss due to fat and protein malabsorption.
Clinical Symptoms of Acute Pancreatitis:
sudden onset of epigastric pain that lasts for hours to days and radiates to the back, nausea and vomiting, sweating, weakness, and anxiety. The patient often feels better when sitting up and leaning forward.
Physical examination findings of Acute Pancreatitis:
The patient may be febrile, tachycardic, tachypneic, and hypotensive. The skin of the periumbilical area may be discolored (Cullen’s sign). Flank ecchymoses (Grey Turner’s sign) may be present. The abdomen may have mild distention (because of ileus). Upper abdominal and epigastric tenderness (usually without rebound or rigidity) is often present.
Laboratory findings of Acute Pancreatitis:
Elevated serum amylase and lipase. Blood amylase or lipase levels are typically elevated three times the normal level during acute pancreatitis.
Other findings may include leukocytosis (12,000–15,000/μL), hypoalbuminemia, hyperglycemia, and elevated aspartate aminotransferase (AST, SGOT), alkaline phosphatase, and bilirubin.
Imaging for Suspected Acute Pancreatitis [but not necessary]:
CT ABDOMEN- PELVIS.
Causes of Acute Pancreatitis:
Biliary stones, Alcohol abuse, Drugs, Hyperlipidemia or Hypercalcemia, Idiopathic or Infectious, Trauma, Surgery (after endoscopic retrograde cholangiopancreatography [ERCP], intra-abdominal surgery) or Scorpion sting.
- Biliary stonesare the most common cause of acute pancreatitis in hospitalized patients.
- Alcohol abuseis the most common cause of pancreatitis overall in the United States.
- Many drugs can cause acute pancreatitis: thiazide diuretics, sulfa antibiotics, pentamidine, and some antiretroviral agents.
- Hyperlipidemia (types I, IV, V).Pancreatitis usually does not occur in hyperlipidemic patients until their serum triglyceride level exceeds 1000 mg/dL.
- Idiopathic causes: possibly due to pancreas divisum (a congenital defect), autoimmune pancreatitis, or microlithiasis as the cause. Pancreatic malignancy can also cause acute pancreatitis.
- Infectious etiologiesinclude mumps, cytomegalovirus (CMV), human immunodeficiency virus (HIV), and infections caused by Escherichia coli.
- Blunt, rather than penetrating, trauma. Blunt trauma may cause ductal disruption, leakage of pancreatic enzymes, and autodigestion of the pancreas leading to pancreatitis.
- Surgical: Postsurgical pancreatitis in patients undergoing ERCP.
- Scorpion stings: Scorpion stings are a common cause of pancreatitis in the Caribbean islands of Trinidad and Tobago.
Ranson’s criteria are used to assess severity and prognosis.
Ranson’s criteria are assessed at admission and during the initial 48 hours.
Ranson’s Criteria During the Initial 48 Hours. Ranson’s greater than 3 is SEVERE.
Base deficit >4 mEq/L
Calcium <8 mg/dL
Hematocrit decrease >10%
Sequestration of fluid >6 L
Oxygen <60 mm Hg
Blood urea nitrogen (BUN) increase of >5 mg/dL
As the number of criteria met increases, so does the mortality rate.
Treatment of Acute Pancreatitis:
- Treatment is primarily supportive and includes bowel rest, aggressive volume resuscitation, pain control, and management of respiratory distress and renal failure.
- Early feeding of patients with pancreatitis (as opposed to prolonged bowel rest) may be associated with improved outcomes.
- Nasogastric tubes are used for gastric decompression in patients with persistent vomiting.
- If gallstones are thought to be the cause, ERCP may be indicated.
- Cholecystectomy should only be considered after the patient recovers from the acute episode.
Complications of Acute Pancreatitis:
- Pancreatic abscess: should be suspected if the patient worsens after initial improvement. Persistent pain and fever are clues to the occurrence of an abscess. Re-image the patient with a CT scan.
- Pancreatic pseudocyst: occurs in 10%–20% of patients.
- Renal failure and respiratory failure are the two most common systemic complications and can be life-threatening.
Alcoholic Hepatitis
3 Histological Stages
- Simple steatosis (usually reversible w/ abstinence in 4-6 wks)
- Steatohepatitis (steatosis + neutrophil infiltration + Mallory-Denk bodies)
- Steato-fibrosis (extreme is cirrhosis)
MELD SCORE [calculate with mdcalc]
Model for End-Stage Liver Disease (MELD) score is a prognostic scoring system used to predict 3-month mortality due to liver disease
MELD scores range from 6 to 40; the higher the score, the higher the 3-month mortality related to liver disease
MDF SCORE [calculate with mdcalc]
Maddrey Discriminant Function (MDF) score is a measure of disease prognosis in alcoholic hepatitis (AH) used to identify patients at highest risk of mortality and determine the need for initiation of pharmacologic treatment.
An acute inflammatory syndrome that develops in the setting of chronic liver inflammation w/ alcohol use.
Risk Factors
Amount of alcohol, duration of alcohol use (>5-10 yrs for cirrhosis), gender (F>M), ethnicity (↑risk in AA & Hispanics), HCV (>30x ↑risk for cirrhosis), genetic mutations (PNLPA3) and obesity
Clinical Presentation
Hepatomegaly, jaundice, ascites, encephalopathy and fever.
Of note: alcohol related hepatitis can lead to portal HTN and varices and ascites in the absence of cirrhosis due to hepatic swelling and portal venous obstruction.
Diagnosis
- Often cholestatic LFTs (↑alk phos) with elevated AST & ALT (usually <300), typically in >2:1 ratio).
- ALT can be normal if vitamin B6 deficiency.
- ↑WBC
Treatment for Alcohol Related Hepatitis
- If MDF ≥ 32 (Or MELD >20) and/or presence of encephalopathy commence steroids: prednisolone 40mg/d for 4 weeks +/- taper x 2-4 weeks. Adding NAC may be beneficial, but ask for GI input before starting. Consider pentoxyfylline if steroids are contraindicated. Consult hepatology for consideration of early liver transplant if appropriate.
- Contraindications to prednisolone: active infection, chronic HBV/HCV, GIB, pancreatitis, renal failure.
- Lille Score: composite score of age, Cr, alb, PT, Tbili on day 0 and Tbili on day 7 of steroids. Calculate on day 7 to evaluate response to steroids; a score >0.56 indicates lack of response at 7 days → can discontinue steroids.
- Supportive therapy: monitor for infection, consider PPI/ H2RA, monitor for signs of HRS and avoid nephrotoxic drugs, hold beta blockers if MDF ≥ 32 due to incidence of AKI.
- Nutrition therapy: MVI, thiamine, folate, enteral feeding; nutrition independently decreases mortality.
- Only abstinence from alcohol and liver transplant are effective for long term treatment of alcohol related hepatitis. At discharge, patients should receive medication assisted therapy (acamprosate 666 mg TID, naltrexone 50mg QD, baclofen 5- 10mg TID, gabapentin 600mg TID)
Nausea
Nausea is the unpleasant sensation of about to vomit. This can occur alone or with vomiting. Many differentials are associated with nausea depending on patient's symptoms.
Always check patients electrolytes if they have been having severe vomiting and replete electrolytes if required. Suggestive labs could include BMP (checking electrolytes), UA (checking for ketones and specific gravity).
Treatment of nausea includes:
- Metoclopramide (Reglan) 10mg po/iv q4hr PRN
- Prochlorperazine (Compazine) 10mg po/im/iv q6hr
- Droperidol 0.625-1.25mg IV/IM q6hr PRN
- Lorazepam (Ativan) 0.5-2.0 mg po/iv q4-6hr PRN
Things to prevent nausea include:
- Ginger ale or chamomile tea to settle that stomach
- Avoiding caffeine that tends to upset stomach
- Drink lots of water and stay hydrated
- Eating small meals to allow your stomach to digest foods slowly
- Avoiding spicy, processed foods
Neuroleptic Malignant Syndrome can be caused by excessive use of Compazine or Droperidol (stop antiemetic and start Lorazepam 1-2mg IV 4-6hrs or Dantrolene 1-2.5 mg/kg IV with max dose of 10mg/kg/day).
Advise all patients that Antiemetics can cause drowsiness
Combination of anti-emetics will resolve patient's nausea if patient is unresponsive to a single medication.
Constipation
Check if patient has Bowel Obstruction before giving anything PO
Stool Softeners - Colace 100-250mg po qd or bid
Osmotic Laxatives
- MiraLAX 17gm daily
- Lactulose 30ml q4hr until bowel movement
- Milk of Magnesia 30ml to 60ml qd
Suppository - Dulcolax 10mg qd, mineral oil enema, fleet enema
Patients started on narcotics should be advised about constipation. Also patient's on chronic narcotics should be on bowel regimen to prevent constipation.