Hematology
Anemia
Anemia can be caused by many things but first we should get some basic labs such as CBC that will show MCV, and Reticulocyte count.
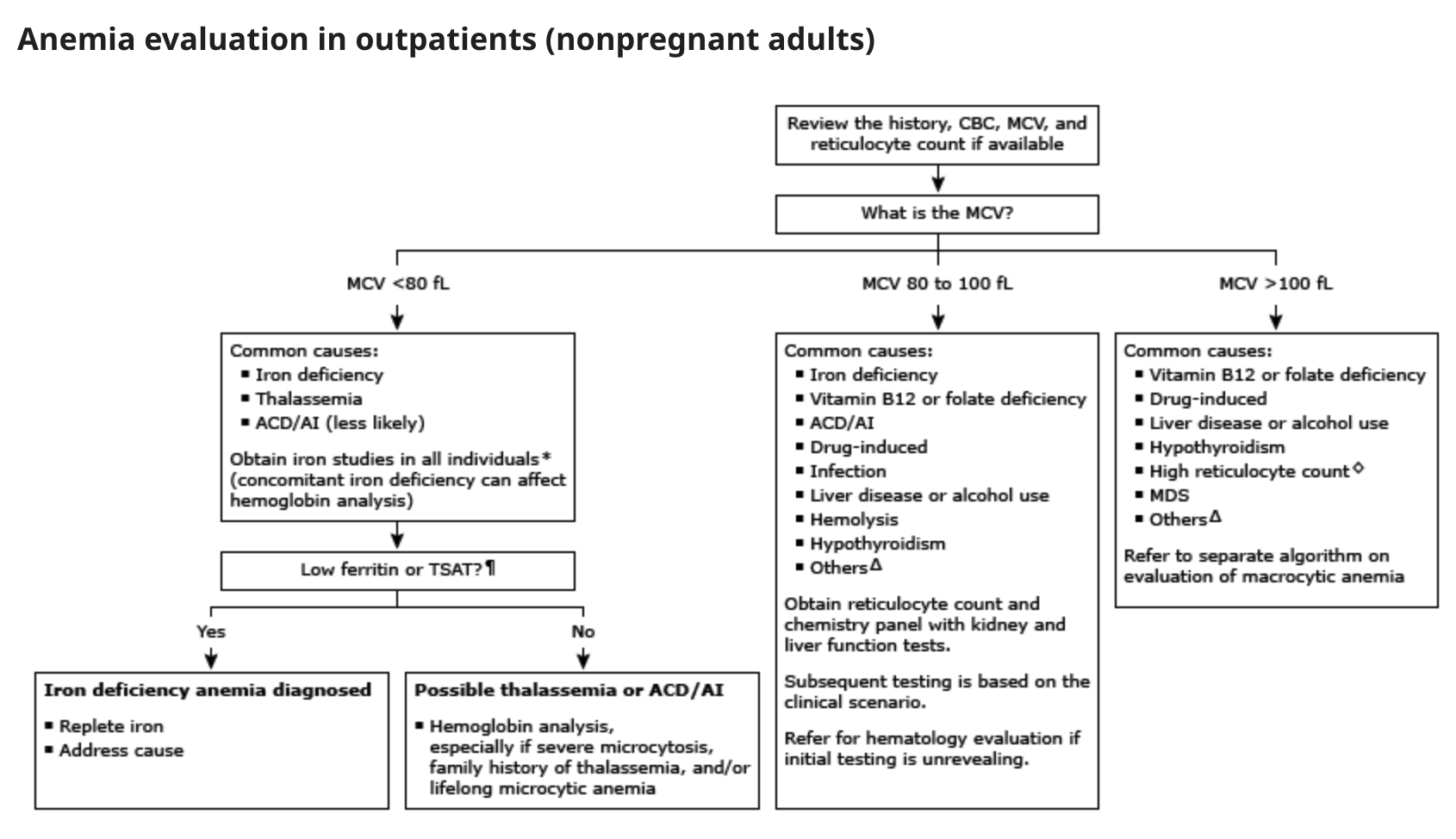

This table from UTD summarizes on the different causes of anemia depending on the MCV.
Increased reticulocyte count (increased red cell breakdown) will also require peripheral smear to narrow differential.
- Acute blood loss
- Hemolysis - including antibody mediated, cellular toxins (malaria, clostridium), trauma (valve), or hypersplenism.
- Intrinsic Defect- including enzyme deficiency such as G6PHD, SCD, or thalassemia
- Membrane Defect- including spur cell, hereditary spherocytosis or PNH
Anemia with decreased reticulocyte count
- Deficiency of Iron, Vit B12, Folate, or copper
- Medication that can suppress the bone marrow (such as quinidine, TMP SMX, albendazole)
- Primary bone marrow disorders (MDS, Myelofibrosis, or leukemia)
- Very recent bleeding (within 5-7 days, before bone marrow compensation has occurred)
If patient has Hgb of <7 in Non cardiac patient or <8 in cardiac patient we should consider blood transfusion (pRBC). (Let the patient know of the risk's and benefits and also inquire that patient is not a Jehovah's Witness before proceeding with blood transfusion).
Sickle Cell Pain Crisis
- Sickled cells occlude arterioles and cause tissue infarction, resulting in recurrent painful episodes, and a variety of serious organ system complications that can lead to life-long disabilities and even death.
- Causes: Precipitated by infection, fever, dehydration, or exposure to low oxygen tension (high altitude travel).
- Clinical manifestations: Characterized by severe pain, typically of the back, limbs, ribs, lasting 5-7 days. Pattern of pain in a given patient usually consistent from crisis to crisis. If new pain, consider an alternative diagnosis.
Treatment:
- Oral hydration with 3-4 liters of fluid per day. We sugest to start 0.5 to 1 L NS bolus, then maintainance D51/2NS at 150-250 cc/hr.
- Pain management: These patients are usually on chronic opioids. Start dose of IV morphine based on patient's prior dose requirements, or start with 2-5 mg morphine every 3-4 hours. Convert to PO once IV dose approaches equal analgesic home regimen. Perform assessments every 20 min and escalate as needed.
- Supplemental O2 if hypoxia is present. Provide incentive spirometry.
- Provide stimulant (not osmotic) laxatives.
- Avoidance meperidine (can precipitate seizures), and ketorolac (associated with AKI).
- Evaluate for SCD complications associated with pain (eg, avascular necrosis of the hip, acute chest pain syndrome, splenic sequestration). CBC, retic count, cultures, lytes, BUN, vreatinine, bilirubin, UA, CXR,blood type and screen.
Blood Component Therapy
Packed red blood cells (PRBC):
WBCs are the chief cause of alloimmunization to HLA antigens, which leads to future febrile transfusion reactions and platelet refractoriness. Indicated for patients who require long term transfusion support (Bone marrow transplant, leukemia, chemotherapy), and are at risk of becoming refractory to platelets, or with recurrent febrile reactions.
Products are irradiated to kill donor stem cells which (rarely) cause transfusion-associated GVHD.
Indicated for BMT recipients, immunosuppressed patients, when donor and recipient are blood relatives, and patients receiving HLA matched platelets.
RBC washed to remove plasma proteins, electrolytes, and antibodies. Indicated only in patients with history of severe transfusion reactions, hyperkalemia, paroxysmal nocturnal hemoglobinuria. Very expensive!
Active bleeding and one of the following:
1 - Blood loss > 500cc or 15% of blood volume (70 cc/kg body weight)
2- SBP < 100 mmHg or 20% fall in SBP
3- Pulse > 100 bpm
4- General anesthesia and Hgb < 9 g/dl
5- Chronic, symptomatic anemia (generally Hgb < 9g/dl)
6- Chronic transfusions to suppress endogenous Hgb in selected patients with sickle cell disease
7- Hgb < 10 g/dl in patients with known coronary artery disease, unstable angina, or acute MI. No RTC trial data to support this practice. One RCT (n=428) in patients undergoing CABG randomized patients to transfusion only if Hgb < 8 g/dL or standard practice (generally Hgb > 9.0) and found no mortality differences.
9- ICU mortality data with clear evidence for more restrictive transfusion (Hgb<7.0) practices
Patients with chronic anemia increase plasma volume in order to maintain an adequate cardiac output.
The volume associated with transfusion will cause overload and must be done slowly to avoid precipitating CHF (4 hours per unit vs. 5-10 min/unit in a hypotensive patient with acute blood loss).
Consider transfusing in splits of ½ volume over same time (4 hours per split is the slowest rate at which blood may be transfused).
Consider Lasix 20-40 mg IV to avoid fluid overload during transfusion of multiple units.
Platelets:
1- 1 unit single donor platelets (SDP) = 7 units of random donor platelets (a hemostatic dose for bleeding in an adult patient)
2- General dose is 1 unit random donor platelets per 10 kg body weight ≈ 1 unit single donor platelets for a 70 kg person.
3- For every 1 unit of SDP, the patient receives hemostatic levels of coagulation factors equivalent to 1 unit of fresh frozen plasma.
1- Platelet count < 5-10K in ITP or significant purpura
2- Platelet count < 10K in J patients, or patients not predisposed to spontaneous bleeding. No change in bleeding events in RCT when compared to < 20K as transfusion threshold
4- Platelet count < 20K and a clinical factor that would be associated with risk of spontaneous bleeding (Temperature > 38.5°C/Infection, concurrent coagulopathy, DIC, hepatic or renal failure, marked splenomegaly)
5- Platelet count < 50K and surgery or post-op bleeding
6- Platelet count < 50K and invasive procedure (LP, indwelling lines, liver or transbronchial biopsy, epidural puncture)
7- Platelet count < 100K with active bleeding
1- Causes: fever, sepsis, splenomegaly, DIC, drugs, platelet consumption, s/p BMT (likely multifactorial etiology, in one series < 40% post-BMT transfusions resulted in appropriate rise in platelet count), alloimmunization with antibody mediated destruction of circulating platelets (towards HLA class I antigen)
2- Diagnosis: check rise 60 minutes after transfusion.
3- Appropriate rise with decrease over next 24 hours®sepsis, DIC, post BMT, etc. No rise at 60 minutes indicates alloimmunization. Order platelet antibody screening test (results in 2-3 days).
4- Treatment: if test positive, or while results pending, order "HLA matched" platelets and check platelet count 10 minutes to 1 hour following transfusion to document appropriate rise. Minimal options in acute bleed situation.
Effort should be made to avoid alloimmunization in at risk patients through irradiation, leukocyte reduction (comparable in RCT) or both.
Fresh frozen plasma (FFP):
FFP is made by separating plasma from a unit of whole blood. Contains all clotting factors. One unit of FFP contains: 200-250 cc volume, 400 mg fibrinogen, 200 units of other factors (factors V, VII, XI, ATIII, Protein C, Protein S)
1- Active bleeding or risk of bleeding if PT and/or PTT> 1.5-1.8x normal.
2- Patient with massive bleeding at high risk for clotting factor deficiency while coags pending. Common causes of factor deficiency: liver disease, vitamin K deficiency, DIC, hemorrhage, TTP (treatment with plasma exchange)
3- Reversal of warfarin therapy. Minimal evidence that FFP can correct mildly elevated INR (< 1.8).
1- Starting dose 15 cc/kg = 4-6 units (dose needed to replace 25% clotting factors, minimum amount necessary to obtain hemostasis)
2- Maximum effect declines after 2-4 hours, so infuse rapidly at time of bleeding or no more than 1 hour prior to anticipated bleeding.
3- Administer fewer units of FFP when transfusing platelets since 1 unit SDP contains equivalent clotting factors to 1 unit FFP.
4- Consider Lasix IV when multiple units FFP given rapidly to avoid fluid overload.
Cryoprecipitate: (Contains fibrinogen, factor VIII, and von Willebrand factor)
1- Fibrinogen < 100 mg/dl (as in DIC)
2- Preparation of topical fibrin glue for surgical hemostasis
Concentrated factor VIII and von Willebrand factor are preferred treatments of Hemophilia A and von Willebrand's disease since cryoprecipitate not virus inactivated, thus carrying a higher risk for virus transmission.
1- Usual starting dose is 10 units. Each unit raises fibrinogen by about 8 mg/dl. Follow fibrinogen levels every 6-8 hours to guide frequency and quantity of administration.
Transfusion Reactions
For all reactions (except mild allergic/uricaria): STOP transfusion, send remaining blood product and fresh blood sample to blood bank)
Acute Hemolysis (caused by ABO incompatibility)
1- Stop transfusion immediately if reaction suspected!
2- Maintain blood pressure and urine output with vigorous NS hydration via new infusion set.
3- Lasix 80-100 mg, or mannitol IV to maintain urine output with goal >100 cc urine/hr.
4- Follow strict I/Os.
5- Close monitoring for any electrolyte abnormalities (hyperkalemia)
Anaphylaxis
Acute Lung Injury
Delayed Hemolysis
Bacterial Contamination
Febrile, Non-Hemolytic Transfusion Reaction
Urticaria