OB/GYN
- Rotation expectations
- Routine Visit Schedule
- Routine Testing Intervals/Schedules
- Pregnancy Dating
- Fetal Well-Being
- Intrauterine Growth Restriction
- Nonstress Testing
- Contraction Stress Test
- Biophysical Profile
- Fetal Heart Rate Monitoring
- Laboratory Values in Pregnancy
- Bishop Score
- Recurrent Pregnancy Loss
- Hyperemesis Gravidarum
- Hypertension in Pregnancy
- Vaginal birth after Cesarean
- Post Dates Management
- Gestational Diabetes
- Twins
- ER precautions in Term Pregnancy
- Medication in Obstetrics
- PAP Smear Referral Guideline
Rotation expectations
Call group (only cover patients of the following):
Dr. Vishwanath
Dr. Dickinson
Dr. Marquez
Dr. Gade
Dr. Matharu
Any unassigned patients
Door Codes:
Sleep Rm 4th floor 611#
6th floor doctors’ lounge 33115
From elevator on 6th floor 425#
From COVID area to 6th floor 425
Expectations:
Round on postpartum patients - 4th floor
Round on Antepartum patients - 6th floor
Cover patients in L&D
See all patients in OB ED - 4th floor
Assist for CSs (Surgery is on 2nd floor close to main elevator)
Read NSTs
Cover GYN consults in ER or floors
Postpartum Rounds
Post Op Fever:
Wind - atelectasis
Water - UTI
Wound - infection
Walk - DVT
Wonder drug - heparin
Woman - mastitis, breast engorgement
Womb - endometritis, pelvic vein thrombophlebitis, TOA
Postpartum Hemorrhage:
Can happen postpartum often!
Pre Delivery Hgb → Post Delivery Hgb
Significant drop is > 2
- Oxytocin 20-80 IU/500ml NS IV infused over 10 mins, then 250ml/hr
- Methergine 0.2mg IM or PO (contraindication: HTN)
- Hemabate 0.25mg IM (contraindication: asthma)
- Misoprostol 200 mcg (up to 3 tabs PR or 1 tab PO)
- TXA 1gm/100ml NS IV over 10 minutes
Post-Partum Counseling
- Breastfeeding or Bottle Feeding? - Takes 3-5 days for milk letdown; longer in c/s patients
- Contraceptive Counseling
A) COC's - wait 3 wks postpartum (early Estrogen increases risk for DVT)
- estrogen may cause decrease milk production if breastfeeding-would not start in house but should not wait for 6 week check to do so
B) Progestins- can give immediately post-partum if desired
- Depo provera 150 mg IM q3 mo-same as above
2. IUD - at other institutions is placed immediately postpartum, but more likely can be placed ANYTIME after delivery
3. MIcronor 0.35 mg pill po qd
Post partum Vaccine
- Rubella - if nonimmune or equivocal, need vaccine]
- If Rh negative - check infant
If infant positive → Rhogam
If infant negative → none
Routine Visit Schedule
The first visit of prenatal care typically occurs in the first trimester. The frequency of follow up is based on the individual needs and assessment of risks.
In General, this is what we follow:
- Risk assessment and patient education is initiated at the first prenatal visit. The discussion during first visit should include scope of care that is provided, past medical, genetic, obstetric history, medications, lab studies, expected course of pregnancy, signs and symptoms to be reported to health care team, anticipated schedule of visits, risk counseling including substance use disorder.
- After initial visit, return visit every 4 weeks for the first 28 weeks.
- After 28 weeks, return visit every 2 weeks until 36 weeks.
- After 36 weeks, return visit weekly until delivery.
- If patient is high risk or having any medical/obstetrical complication, patient may be seen sooner.
Remember to always check fetal heart tone with doppler for every pregnant visit especially >12 weeks
Remember urine dip EVERY VISIT!
Start measure the fundal height of uterus after 20 weeks (expect approx 1cm fundal height growth per week of gestation)
Guidelines to Perinatal care Chapter 6
Routine Testing Intervals/Schedules
Initial Visit or First trimester visit:
- Prenatal Panel: CBC, GC/Chlamydia, HIV, Rubella, RPR, HBsAg, UA, Urine culture, Blood type, Rh (D), Antibody
- First trimester screening between 10 weeks to 13 6/7 weeks of pregnancy
- Pap smear at 21 y.o and older, if indicated
- First trimester ultrasound
- Assess risk factors and if positive risk factors consider:
- Referral to perinatologist
- Fully integrated prenatal screening, 1hr GCT, PIH panel, TSH, TB testing, Microalbumin urine or 24hr
- Vaccine: Flu in season, IMPRESS need for COVID vaccination as early in pregancy as possible
- Counseling: Diet/Exercise/Meds/Breastfeeding (EVERY VISIT for BF'ing)
14 to 20 weeks:
- 2nd trimester screening and AFP (15 0/7-19 6/7 weeks)
- Sono: 2nd TM US (18-24) for anomalies and growth
- Vaccine: flu in season
20 to 32 weeks:
- Labs: Repeat CBC and RPR for 2nd TM
- Glucose Tolerance Test after 24 weeks
- RhoGam at 28 weeks, after repeat testing for antibodies
- Vaccines: flu in season, Tdap at 27+ weeks
- Counseling: Kick count and PTL precautions at 28 weeks onwards
32 to 36 weeks:
- Vaccines: flu in season, Tdap if not received already
- Labs: Rpt CBC, GC/chlamydia, RPR during third TM
- Sono: if needed for placental location
- Fetal position (vertex or breech)
- Hospital registration at 34+ weeks
- Fill out BTL consent in cases of desired sterilization with c-section. Send a copy to L&D
- Counseling: Epidural/Lactation/Contraceptives
36 to 40 weeks:
- Send GBS
- Start NST monitoring at 40 weeks
- Set proper expectations for induction at 38-39 weeks and consider induction at 40-41 weeks
Perinatal Care Chp 6. Page 159
Prenatal Genetic Screening Test
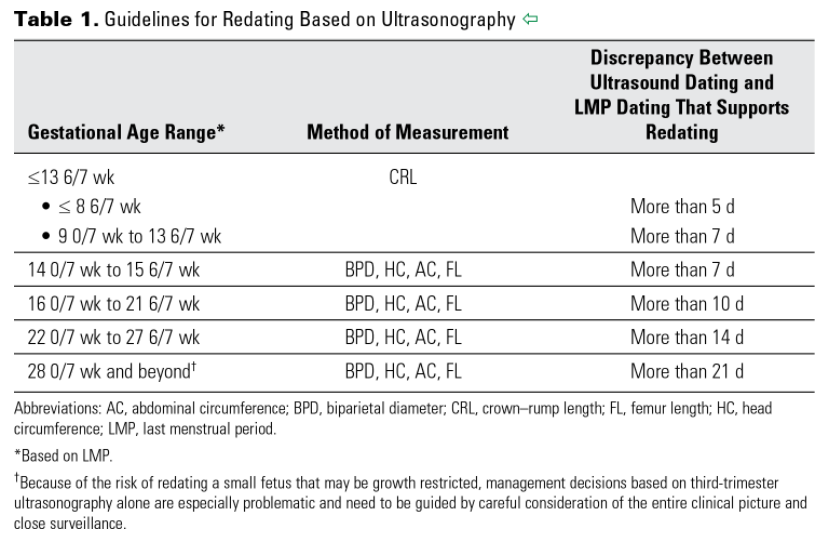
Pregnancy Dating
Step 1: Document First day of the last normal menstrual period then use Nigel's rule or use uptodate EDD calculator to estimate EDD
-
If pregnancy resulted from assisted reproductive technology (ART), the ART-derived gestational age should be used to assign the estimated due date (EDD). For instance, the EDD for a pregnancy that resulted from in vitro fertilization should be assigned using the age of the embryo and the date of transfer.
Step 2: Compare with EDD from first TM ultrasound. Look at Table 1 to see if we should use EDD based on LMP or US
-
Ultrasound measurement of the embryo or fetus in the first trimester (up to and including 13 6/7 weeks of gestation) is the most accurate method to establish or confirm gestational age.
Step 3: Determined EDD
- As soon as data from the last menstrual period (LMP), the first accurate ultrasound examination, or both are obtained, the gestational age and the EDD should be determined, discussed with the patient, and documented clearly in the medical record.

-
A pregnancy without an ultrasound examination that confirms or revises the EDD before 22 0/7 weeks of gestational age should be considered suboptimally dated.
Fetal Well-Being
These are ways used to establish fetal well being:
- Fetal movement count
- Non-stress test
- Contraction stress test
- Amniotic fluid index
- BPP
- Fetal survey for anatomy and growth
- Umbilical artery doppler velocimetry
These test are used to follow:
- GDM
- IUGR
- Chronic hypertension, Pregnancy induced hypertension, preeclampsia
- Polyhydramnios or Oligohydramnios
- Multiple gestations
- >40 weeks gestation
- Any fetus at risk of hypoxia
- Change in fetal movement as perceived by the patient
- Maternal thyroid disease
- Previous stillbirth
- Fetal anomalies
ACOG Guidelines on Antepartum Fetal Surveillance
Intrauterine Growth Restriction
Definition
Sonographic EFW <10th percentile
Etiology
Maternal factor: Behavioral (smoking, substance use, decrease nutritional intake), Medical (Diabetes, HTN, renal insufficiency, autoimmune), extreme of maternal age
Fetal factor: Chromosomal or genetic cause, fetal infection, multiple gestations
Physical examination
Suspect if fundal height < dates or poor maternal weight gain
Magagement
- Growth ultrasounds every 2-3 weeks
- Antenatal testing
- twice weekly NST to once weekly BPP with NST or weekly NST with weekly AFI
- Umbilical artery doppler weekly
- Perinatology consult and consider delivery if poor NST/AFI/BPP , abdominal circ <4 wks biparietal diameter, oligo or doppler umbilical artery end diastolic flow zero or reversed
Pocket Obstetrics and gynecology by K Joeph Hurt 2nd edition
Nonstress Testing
Contraindications:
Gestational age <24 weeks
Interpretation:
>32 weeks
Reactive NST: two fetal heart rate accelerations within a 20-minute interval, peaking at least 15 beats per minute above the base line and lasting 15 seconds
<32 weeks
Reassuring for gestational age: two fetal heart rate accelerations 10 beats above the baseline and lasting for 10 seconds within a 20-minute interval.
Contraction Stress Test
The contraction stress test is interpreted by the presence or absence of late fetal heart rate decelerations.
-
Negative: No late or significant variable decelerations.
-
Positive: Late decelerations following 50 percent or more of contractions (even if the contraction frequency is fewer than three in 10 minutes).
-
Equivocal-suspicious: Intermittent late decelerations or significant variable decelerations.
-
Equivocal-hyperstimulatory: Fetal heart rate decelerations that occur in the presence of contractions that are more frequent than every two minutes or last longer than 90 seconds.
-
Unsatisfactory: Fewer than three contractions in 10 minutes or a tracing that is not interpretable.
Relative contraindications to the contraction stress test usually include conditions that are associated with an increased risk of preterm labor and delivery, uterine rupture or uterine bleeding.
Biophysical Profile
Scoring: The non stress test (2), fetal breathing movement (2), Fetal tone (2), Fetal movement (2), amiotic fluid (2)
-
Eight to ten is usually considered normal.
-
Six is considered equivocal (uncertain).
-
Four or less is considered abnormal.
- To get 2 points of breathing : one or more episodes of rhythmic fetal breathing movements of 30 seconds or more within 30 minutes)
- To get 2 points of movement: three or more discrete body or limb movements within 30 minutes
- Fetal tone: one or more episodes of extension of a fetal extremity with return to flexion, or opening or closing of a hand
- Amniotic fluid: a single vertical pocket of amniotic fluid exceeding 2 cm is considered evidence of adequate amniotic fluid
The modified BPP combines the nonstress test and an evaluation of the amount of amniotic fluid called the amniotic fluid index (AFI).
The largest pocket of amniotic fluid is measured in each of the four quadrants of the mother's abdomen using ultrasound. All four quadrants added together give the amniotic fluid index.
- AFI: < 5: oligohydramnios ; >25: polyhydramnios
Fetal Heart Rate Monitoring
BASELINE FHR
The normal FHR range is between 120 and 160 beats per minute (bpm). The baseline rate is interpreted as changed if the alteration persists for more than 15 minutes.
FHR VARIABILITY
Prematurity decreases variability therefore, there is little rate fluctuation before 28 weeks. Variability should be normal after 32 weeks.
Beat-to-beat or short-term variability is the oscillation of the FHR around the baseline in amplitude of 5 to 10 bpm.
Long-term variability is a somewhat slower oscillation in heart rate and has a frequency of 3 to 10 cycles per minute and an amplitude of 10 to 25 bpm. Clinically, loss of beat-to-beat variability is more significant than loss of long-term variability and may be ominous.
Decreased or absent variability should generally be confirmed by fetal scalp electrode monitoring when possible.
Increased variability in the baseline FHR is present when the oscillations exceed 25 bpm. This pattern is sometimes called a saltatory pattern and is usually caused by acute hypoxia or mechanical compression of the umbilical cord.
FETAL TACHYCARDIA
Baseline heart rate greater than 160 bpm and is considered a non-reassuring pattern. Mild when the heart rate is 160 to 180 bpm and severe when greater than 180 bpm.
FETAL BRADYCARDIA
Fetal bradycardia is defined as a baseline heart rate less than 110 bpm.
Bradycardia in the range of 100 to 110 bpm with normal variability is not associated with fetal acidosis. Bradycardia of this degree is common in post-date gestations and in fetuses with occiput posterior or transverse presentations.
Moderate bradycardia of 80 to 100 bpm is a nonreassuring pattern.
ACCELERATIONS
The presence of at least two accelerations, each lasting for 15 or more seconds above baseline and peaking at 15 or more bpm, in a 20-minute period is considered a reactive NST.
EARLY DECELERATIONS
Early decelerations are caused by fetal head compression during uterine contraction, resulting in vagal stimulation and slowing of the heart rate. This type of deceleration has a uniform shape, with a slow onset that coincides with the start of the contraction and a slow return to the baseline that coincides with the end of the contraction.
LATE DECELERATIONS
Late decelerations are associated with uteroplacental insufficiency and are provoked by uterine contractions. Any decrease in uterine blood flow or placental dysfunction can cause late decelerations.
A late deceleration is a symmetric fall in the fetal heart rate, beginning at or after the peak of the uterine contraction and returning to baseline only after the contraction has ended
VARIABLE DECELERATIONS
Variable decelerations are shown by an acute fall in the FHR with a rapid downslope and a variable recovery phase.
https://www.aafp.org/pubs/afp/issues/1999/0501/p2487.html
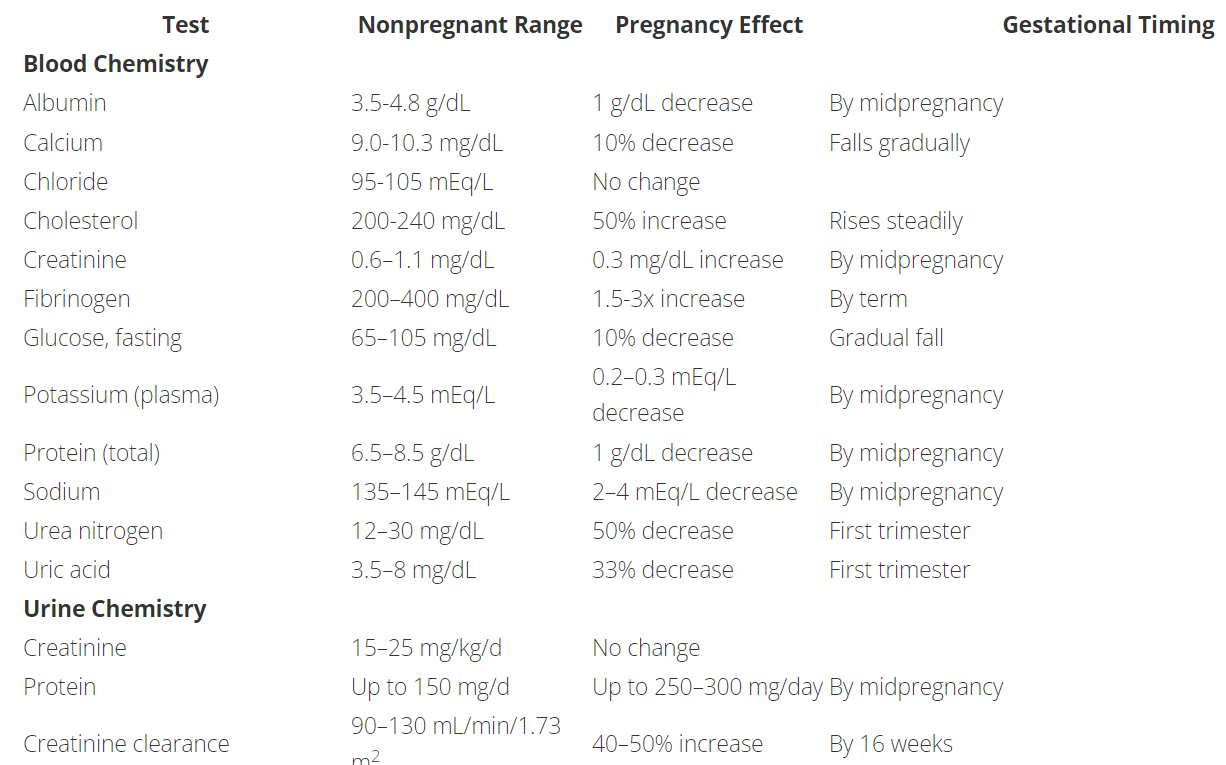
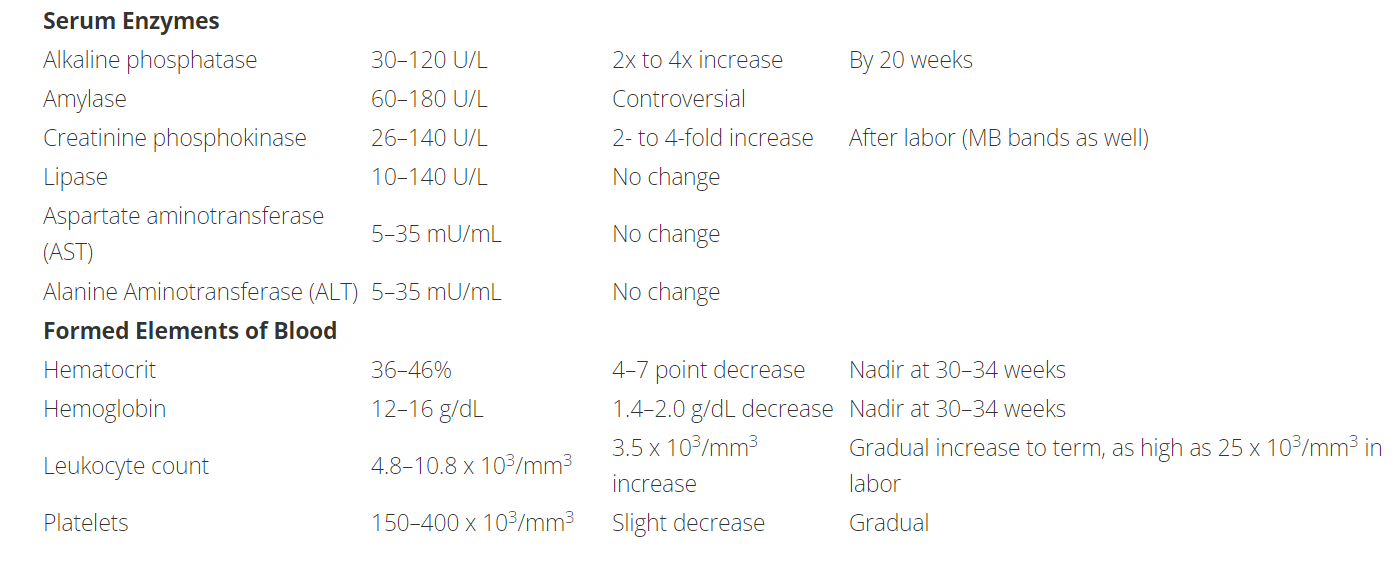
Laboratory Values in Pregnancy
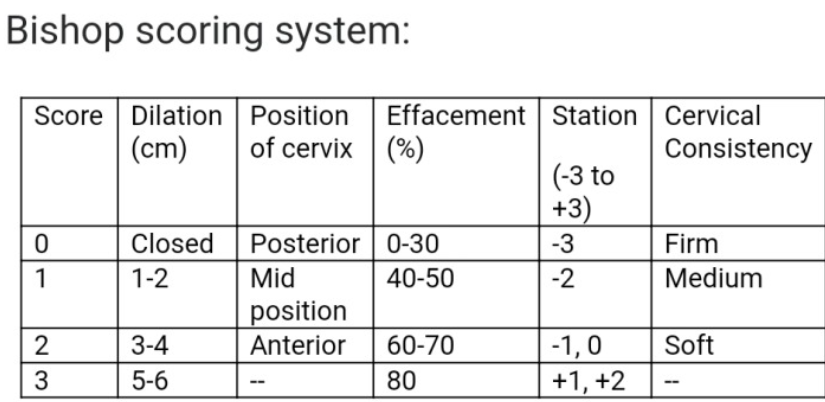
Bishop Score
The Bishop score may be used to rate the readiness of the cervix for labor.
- Scores ≤ 5 suggest an unfavorable cervix, and that induction may be necessary for successful vaginal delivery.
- Scores 6-7 do not definitively predict whether or not induction will be successful. Consider induction or augmentation of labor based on clinical judgment.
- Scores ≥ 8 suggest spontaneous vaginal delivery is more likely and augmentation or induction may be unnecessary
Recurrent Pregnancy Loss
Definition
3 or more consecutive preg losses before 20wk gest or after 2 consecutive losses, esp if age >35 y.o
Evaluation
- Determine actual gestational age at time of miscarriage rather than time of onset sx
- Ask about hx of thrombosis or prev fetal death, dysmenorrhea or menorrhagia ; chronic medical conditions such as thyroid dz, diabetes, or autoimmune dz such as lupus; smoking, toxins, obesity, EtOH use, excessive caffeine use
Diagnostic Workup
- Genetic (parental)
- Antiphospholipid Ab w/u: Lupus anticoagulant, beta 2 glycoprotein Ab (IgM/IgG) and anticardiolipin Ab (IgM/IgG). Need 2 positive tests 6-8weeks apart to make dx
- Consider thrombophilia w/u only if patient has a hx of thromboembolism. Test for favtor V Leiden, prothrombin G20210A mutation, protein C/S, antithrombin III deficiency
- Evaluate uterine cavity using pelvic US, hysteroscopy
- No dx is made in 50% of cases of recurrent pregnancy loss
Pocket Obstetric and Gynecology by K Joseph Hurt, 2nd edition
Hyperemesis Gravidarum
Definition
Nausea and vomiting in pregnancy that significant enough to cause dehydration, metabolic alkalosis, ketonuria, weight loss (>5%), hypokalemia
Risk Factors
Multi gestation, Family history or personal hx in prior pregnancy
Labs
CBC, lytes, UA, TSH, LFT
Therapy
IV hydration with dextrose +/- thiamine
hospitalization for monitoring
Pharmacotherapy
Diglecis
Ondansetron 4 to 8 mg q8hr
Promethazine 12.5 to 25 q4-6hr
Metoclopromide 5 to 10mg q8hr
Diet
Usually begin with a diet consisting of bananas, rice, applesauce and toast (BRAT diet) and then advance the diet as tolerated.
Hypertension in Pregnancy
Definition
Chronic HTN: SBP greater equal to 140 or DBP greater equal to 90 prior to 20 weeks or persisting longer than 12w post partum
Gestational HTN: SBP greater equal to 140 or DBP greater equal to 90 after 20 weeks with or without proteinuria
Pre-eclampsia: New onset HTN (SBP >140 or DBP >90 x2 greater than 4hrs apart) with proteinuria more than 20 weeks. Proteinuria defined as >300mg/24hr (or 1+ urine dip or urine protein:creatinine ration of >0.3). If severe features are present, proteinuria is NOT needed for the diagnosis.
Severe features: SBP >160 or DBP >110; thrombocytopenia <100,000; elevated liver enzyme test more than 2x upper limit of normal, severe RUQ pain, renal insufficiency (cr >1.1 or doubling of baseline value); pulmonary edema; new onset cerebral/visual sympmtoms
Eclampsia: Pre-eclampsia with seizures
Diagnostic work up
CBC. CMP (evaluate liver and renal function), assessment of proteinuria (by urine spot prot to creatinine ratio, UA, or 24h urine collection)
Treatment and Medication
Acute HTN
Labetalol: 20mg IV, rpt at 10 min intervals, double dose with max dose of 80mg at 1 given time; total max dose of 300mg
Hydralazine: 5-10mg IV over 1-2 min, rpt a 20 mins interval. Max dose of 30mg
Nifedipine: 10mg PO, rpt at 20 min interval. If next BP severe, can give 20mg PO
Nitroprusside: 0.20-4mcg.kg.min IV drip, titrate to effect. Only in critical illness
Nicardipine: 2.5mg/h IV titrating, do not exceed 15mg/h
DO NOT USE: ACEI or ARB
Oral treatment
Labetalol: 100-800mg PO BID-TID (Max dose 2400mg/24hr)
Methyldopa: 250 mg PO BID (Max dose 3g/24hr)
Nifedipine XR: 30-90 mg PO daily (Max dose 120mg/24h)
Pre-Eclampsia with severe features or chronic HTN with superimposed pre-Eclampsia with severe features
Magnesium sulfate for seizure prevention: Given during stabilization prior to expectant management, during delivery, and 24h postpartum. Bolus 4-6g IV with maintenance of 1-2g/h for seizure prevention, titrate and consider no bolus if pt has renal failure. Monitor closely for pulm edema as MgSo4 is a smooth muscle relaxer
Timing for delivery:
Chronic HTN: No earlier than 38w if well controlled
Gestation HTN: 37weeks
Pre-Eclampsia
- Without severe feature: 37 weeks or >34 weeks if IUGR
- With severe feature: at 34 week if severe HTN is only feature. Otherwise deliver after 48hr of steroid if other severe feature present
Chronic HTN with superimposed preeclampsia: at 37 week if no severe features. Otherwise same as preeclampsia with severe feature
Pocket Obstetric and Gynecology by K Joseph Hurt, 2nd edition
Vaginal birth after Cesarean
Appropriate candidates
Hx 1-2 C-section via low transverse hysterotomy.
Inappropriate candidates
Previous classical or T-incision, prior uterine rupture, extensive transfundal uterine surgery (ex: myomectomy), and patient with any contraindication to vaginal delivery.
Online NICHD VBAC success rate calculator
Delivery Considerations
- Misoprostol should NOT be used for TOLAC induction given elevated risk of uterine rupture
- Continuous fetal monitoring should be employed
- Maintain high suspicion for signs/sx of uterine rupture, including new onset uterine pain, loss of fetal station, new fetal heart race tracing abnormalities (most common), vaginal bleeding and maternal hemodynamic instability
- Staff (OB and anesthesia) must be immediately available for emergent c-section
Pocket Obstetrics and gynecology by K Joeph Hurt 2nd edition
Post Dates Management
- Review gestational dating
- AFI/BPP and NST at 41 weeks and repeat once to twice a week
- Consider membrane stripping at 39 weeks
- Consider induction at 41 weeks and cervical ripening agents
Gestational Diabetes
Universal screening start at 24-248 weeks.
Consider screening earlier in all women with BMI >25 and one or more risk factors:
- Physical inactivity
- 1st degree relative with DM
- High-risk ethnicity (AA, Latino, NA, Asian, Pacific Islander)
- Previous GDM or previous more than equal to 4000g birth
- Hypertension
- PCOS
- Prepregnancy BMI >40
Screening test:
1hr OGTT (50g): serum >130-140 , Positive screening test -->3hr OGTT (100g)
3hr OGTT (100g): Fasting plus 1hr, 2hr, 3hr. 2 or more abnormal values = GDM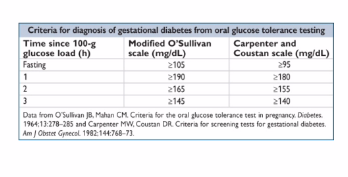
Management
- Nutrition advise, diet/exercise and 4x/day blood glucose testing (fasting + 2hr postprandial). Goals for fasting 60-90 ; 2hr post prandial : <120
- If inadequate control --> insulin (NPH q12h with preprandial short acting insulin 3-4 x daily) 0.7-2u/kg current patient weight . Oral agents used much less these days (glyburide and metformin)
- Insulin management: with active labor or gluc <70mg/dL start D5NS IVF, check fingerstick glucose qhourly. Usually pregestational DM --> IV insulin drip and titrate
- NST once or twice weekly starting at 32 weeks for controlled on medication without severe feature
- NST twice weekly starting at 32 weeks for poorly controlled
- Delivery 39-40w unless poorly controlled
- Consider C-sec for EFW >4500g
- GDM resolves with delivery so do post partum 75g glucose (2h OGTT) at 6 weeks post partum to identify non-gestational DM for all GDM patients
Pocket Obstetrics and gynecology by K Joeph Hurt 2nd edition
Twins
At risk for hyperemesis, GDM, HTN, hemorrhage, cesaeran, postpartum depression, preeclampsia, preterm delivery, IUGR, birth/genetic defects
- Pre-term labor education
- Fetal kick count starting at 28 weeks (10 kicks/movement within 2hrs or less)
- NST weekly starting at 36 weeks for uncomplicated dichorionic
- NST weekly starting at 32 weeks for uncomplicated monochorionic diamniotic.
Management
- Dichorionic twins
- Early US for chorionicity, detailed US at 18-22 wks, growth every 4-6 weeks, delivery at 38 weeks
- Monochorionic diamniotic twin
- Early US for chorionicity, US for TTTS (twin to twin transfusion syndrome) f/u every 2 weeks at 16 weeks, growth every 4 weeks, delivery at 34-37 weeks
- Consults with perinatologist for discordant growth, monoamniotic twins (cord accidents) or monochorionic twins (twin to twin transfusions)
Pocket Obstetrics and gynecology by K Joeph Hurt 2nd edition
ER precautions in Term Pregnancy
- Regular painful contraction every 5 minutes (nulliparous) or every 10 minutes (multiparous), or sooner if long distance to hospital or history of precipitous delivery
- Rupture of membrane
- Vaginal bleeding
- No or decreased fetal movement (<10 kicks in 2hrs)
Medication in Obstetrics
Minimize all medication use during pregnancy (especially in 1st TM), unless clearly indicated!
FDA pregnancy categories
A: No risk in controlled human studies
B: No risk in controlled animal studies and no risk seen in humans
C: Small risk in controlled animal studies, but not seen or not studied in humans
D: Strong evidence of risk in humans but benefit may outweigh tisk
X: High risk - never to be used in pregnant humans
Analgesics
- Acetaminophen - B / compatible with breastfeeding
- Ibuprofen - C 1st/2ndTM ; D 3rdTM / compatible with breastfeeding
- Fentanyl - C / compatible with breast feeding
- Hydromorphone (Dilaudid) - C / compatible with breast feeding
- Morphine - C / Compatible with breast feeding
- Oxycodone (Percoset) - B / Compatible with breast feeding
- Hydrococone (Vicodin) - C / Compatible with breast feeding
Antibiotics
- Ampicillin - B / Compatible with breast feeding
- Amoxicillin - B / Compatible with breast feeding
- Cefazolin - B / Compatible with breast feeding
- Gentamicin - D / Compatible with breast feeding
- Clindamycin - B / Avoid if possible in breast feeding, monitor infant
- Cipro - C (avoid in pregnancy) / Avoid if possible in breast feeing, monitor infant
- TMP-SMX - D / infant risk minimal in breast feeding
- Nitrofurantoin - B in 1st and 2nd TM ; D in 3rd TM / Compatible with breast feeding
- Ceftriaxone - B / Compatible with breast feeding
- Zosyn - B / Compatible with breast feeding
- Erythromycin - B / infant risk minimal in breast feeding
- Vanco - C / infant risk cannot be ruled out in breast feeding
- Keflex - B / Compatible with breast feeding
- Flagyl - B / Infant risk cannot be ruled out, avoid if possible in breast feeding
- Doxycycline - D / avoid in breast feeding
Anticoagulation
- Lovenox - B / Compatible with breast feeding
- Heparin - C / Compatible with breast feeding
- Warfarin - X / Compatible with breast feeding
Antiemetics
- Vitamin B6 - A / Compatible with breast feeding
- Doxylamine - C / May decrease breastmilk supply
- Prochlorperazine - C / Infant risk cannot be ruled out in breast feeding
- Metoclopromide - B / Infant risk cannot be ruled out in breast feeding
- Ondansetron - B / Infant risk cannot be ruled out in breast feeding
- Promethazine HCl - C / Compatible with breast feeding
Diabetes medication
- Metformin - B / Compatible with breast feeding
- Sulfonylurea - B / infant risk cannot be ruled out
- Insulin - B / Compatible with breast feeding
Hypertension or preeclampsia treatment
- Hydralazine - C / Compatible with breast feeding
- Labetalol - C / Compatible with breast feeding
- Magnesium sulfate - A / Compatible with breast feeding
- Nifedipine - C / Compatible with breast feeding
Psychiatric / substance abuse medications
- Zolpidem - C / Caution with breastfeeding
- Buproprion - C / Compatible with breast feeding
- Citalopram, fluoxetine, Sertraline - C / Compatible with breast feeding
- Trazodone - C / Compatible with breast feeding
- Lorazepam - D / Compatible with breast feeding
https://www.aafp.org/afp/2003/0615/p2517.html
Pocket Obstetric and Gynecology by K Joseph Hurt, 2nd edition