HouseStaff Handbook
This highlights key topics that all SAMC Family Medicine residents are recommended to acquire during their residency training. The topics included are routinely updated to reflect guideline changes and best practice recommendations. Other nuance topics that pertains to inpatient and outpatient rotations are included for guidance and expectations. Please utilize this handbook during your rotations.
- General Information
- How To
- Inpatient Service
- Common Calls From The Floor
- Bradycardia
- Tachycardia
- Hypotension
- Hypertension
- Fever
- Low urine output
- Dyspnea
- Chest pain
- Combative or Confused patients
- Falls
- Insomnia
- Acid/Base And Electrolytes
- Hyponatremia
- Hypernatremia
- Hypokalemia
- Hyperkalemia
- Hypomagnesemia
- Hypermagnesemia
- Hypocalcemia
- Hypercalcemia
- Hypophosphatemia
- Hyperphosphatemia
- Algorithm For Acid Base Disorders
- Assessment Of RTAs
- Cardiology
- Endocrinology
- Gastroenterology
- Hematology
- Infectious Disease
- Neurology
- Pulmonary
- CAP
- Asthma/COPD Flare
- Oxygen Therapy
- ARDS/Mechanical Ventilation
- Stepwise approach to managing Asthma
- Nephrology
- Newborn Service
- Toxicology
- ETOH Intoxication
- Acetaminophen Overdose
- Salicylate Overdose
- TCA Overdose
- Cocaine Overdose
- Opiate Overdose
- Carbon Monoxide Inhalation
- OB/GYN
- Rotation expectations
- Routine Visit Schedule
- Routine Testing Intervals/Schedules
- Pregnancy Dating
- Fetal Well-Being
- Intrauterine Growth Restriction
- Nonstress Testing
- Contraction Stress Test
- Biophysical Profile
- Fetal Heart Rate Monitoring
- Laboratory Values in Pregnancy
- Bishop Score
- Recurrent Pregnancy Loss
- Hyperemesis Gravidarum
- Hypertension in Pregnancy
- Vaginal birth after Cesarean
- Post Dates Management
- Gestational Diabetes
- Twins
- ER precautions in Term Pregnancy
- Medication in Obstetrics
- PAP Smear Referral Guideline
- PEDS
- Immunization Schedule
- ACLS Protocols
- Outpatient Service
- Screening Schedule
General Information
Food
Free lunch at physician lounge West wing first floor (Code 135). Need to show ID Badge.
Lunch hours:
Monday - Thursday 11.30am to 2pm
Fridays - 11.30am to 1:30pm
One Main cafetaria and grill (first floor)
You can pay with your badge money
Hours: Monday to Sunday
Breakfast 6am - 11am
Lunch 11am - 1.30pm for chef table ; Grill 11am - 4pm
Dinner 5pm - 7.30pm for chef table and grill
Grill will reopen again from 8.30pm to 11.30pm
Cyber cafe Starbucks (2nd floor)
Hours : Monday to Friday from 6am to 2pm
You can pay using your badge money
Parking
Hospital Parking
Park in the parking garage. Usually the gate open before 7AM but when it's closed, you will need your badge to open the gate. DO NOT park in the physician parking area or you will get ticket.
MAP (see Legend 6)
Northwest Clinic Parking
4770 W Herndon Ave, Suite 110
Fresno, CA 93722
(559) 450-0463
(559) 450-0464 (fax)
Use badge to access front side entry on clinic facility. Parking is available for physicians and staff on the east facing lot as marked.
Library
It is located on the 2nd floor near the Starbucks cafe, North Wing. Badge access is necessary. Assistance to literature resources and references for research is provided.
Online assistance to OPEN-Athens, Pubmed, and UptoDate setup
Monday-Friday
Librarian: Judith J. Kammerer
judith.kammerer@samc.com
8:30 a.m.-4 p.m
(559) 450-3322
(559) 450-3315 (fax)
Important Door Codes
Our Rounding room : 085#
Sleeping Quarter: 4th floor 611#
6th floor doctors’ lounge 33115
From elevator on 6th floor 425#
From COVID area to 6th floor 425
ED lounge and bathroom code 5051#
Sick, PTO, and Emergencies
If you need to take a sick day, PTO, and other emergencies, please contact our program coordinator via doc halo/email (doc halo faster), and please inform your attending that you are sick or have other emergencies. If it happens during our clinic days, then you need to also inform Eileen Robles (office coordinator), Dr. Kim and Dr. Ruelan so that they are aware and can reschedule your patients.
How To
Call Schedule AMION
- go to Amion.
- Click secure login
- Type password: saintagnes
- When you need to make a consult and wants to know the attending on call, click on the pink arrow on the top left of screen
- To consult nephrology on call during inpatient, dial 559-960-0010
- To see the schedule for the residents and attending on call for our program, click on the "call". The jeopardy residents, PCC resident and PCC attending also can be found here
- To see the residents in the clinic and preceptors, click "clinic" tab
Login for all departments
saintagnes
Login for FM department
samcgme!
Didactics
Didactics is scheduled every Wednesday starting at 1PM
Location is Nursing conference in 1st floor West Wing near the endoscopy. Virtual MS Teams link will be streamed and recorded at:
Virtual Didactics TEAMS Link
Lecture Slides, Materials Access Link
Grand rounds are held either on MS Teams or Nickerson. Please check email notifications.
View GOOGLE Didactics Calendar
Download the iCal format to native mobile App
You are required to Sign-In for attendance
Inpatient Service
Signouts
-
Signouts occur at 7am and 7pm promptly on a daily basis. Do NOT be late.
-
CORES on the EMR should be updated daily.
-
As an intern, you are responsible for your patient’s sign out and you are to be present during all of sign out to listen in case of cross-coverage.
-
As a senior, you are responsible to know all the patients and you are there to step in when interns need help.
Call Days
- CALL days are designated as Monday’s and Fridays. Usually interns will do 24 hour shift on these days. Please refer to AMION for schedule.
- These are days when the most admissions will occur, you are to see them in a timely fashion while still rounding on already admitted patients.
- Seniors will be taking the admissions and distributing to Interns.
Admission Orders
- Place admit order within 1 hour
- Go see the patient
- Do Medical reconciliation
- Place appropriate general orders
- Present and see the patient with your attending
- Modify orders as appropriate
- Repeat for next admit and curse the heavens that it arrived so soon
Procedure Notes
- Perform the procedure
- Find the appropriate procedure note in the EMR
- Complete the procedure note
- Sign and send the note to the attending you did the procedure with
Death and Documentation
- When called for a patient’s death, ascertain that the patient is unresponsive to verbal and tactile stimuli without spontaneous respirations (visually and by auscultation), is pulseless and without heart sounds, and that pupillary reactivity is absent. Furthermore, ensure that you have the correct name by ID bracelet.
- Notify the attending MD, unless the death was expected and you were specifically informed that this wasn’t necessary.
- Notify the next of kin and determine whether an autopsy is desired, also determine whether the family would like to view the body prior to transport to the morgue. It may help the family member to inform them that the patient died peacefully, etc., if this was the case. Have the family sign the release of body (even if they have not yet made funeral arrangements), autopsy request/refusal, valuables forms. Do this ASAP so the family can grieve in peace.
- Call the coroner according to the reasons below. If in doubt, call the coroner. If a case is felt to be a coroner case, neither you nor the family may touch anything immediately surrounding the patient. It is considered tampering.
- Fill out the discharge summary, discharge orders, death note in the chart, death certificate which must be done by a licensed physician (if death is imminent for one of your patients, please leave a completed discharge paperwork upon signout as a courtesy to your colleagues). Ask the nurses for help.
Deaths reportable to Coroner (California Government Code section 27491)
- If patient has not been seen by a physician (or palliative care RN) in the past 20 days
- If death <24hr in hospital
- Suspected criminal act
- Accidental poisoning
- Controlled substance
- Occupational disease
- Contagious disease as the cause of death
- Death in OR or not fully recovered from anesthesia
- Prisoners (in custody)
- Unidentified people
- Cases where physician is unable to state the cause of death.
Common Calls From The Floor
Bradycardia
Evaluation
- Check if the patient is stable or unstable
- Get a complete set of vital signs and EKG
- If concerned, have pacer pads and atropine at the bedside (if unstable, see ACLS bradycardia)
- Determine whether this is sinus bradycardia based on EKG
- Take history and examine the patient, pay attention to symptoms, vital sign abnormalities, and mental status (often be the result of a vagal event from pain, vomiting, or recent surgery)
- Evaluate the medication list and obtain an electrolyte panel, especially potassium, TSH if not done recently and a troponin to evaluate for an ischemic etiology
Management
- Ensure that atropine and pacer pads are easily available
- If unstable follow ACLS protocol for temporary pacing
- Treat the underlying conditions
- Atropine 0.5mg IV repeat every 3-5 minutes max 3mg is first-line for symptomatic/unstable bradycardia
- Medication is a common cause of bradycardia in the hospital particularly beta-blocker and CCB. Consider reversal agent for beta-blocker use IV glucagon and for CCB use IV calcium gluconate
- Transcutaneous pacing is uncomfortable and a transition to temporary transvenous pacing wire should be made if continuous pacing for >12hrs is anticipated. These patients should be transferred to the ICU and cardiology should be consulted
Tachycardia
Narrow complex tachycardia
Evaluation
- Obtain EKG and complete set of vital sign to check for hemodynamic instability
- If unstable follow ACLS protocol
Management
- Unstable: follow ACLS protocol and do not delay synchronized cardioversion
- Try vagal maneuver or adenosine.
- Vagal maneuver:
- Valsalva
- Carotid massage
- Adenosine: Warn patients that adenosis will make them feel terrible but it will be short.
- Dosing:
- Peripheral IV 6mg x1. may repeat one more time with the same dose several minutes later if not improving, then increase to 12mg dose x1
- Central line: 3mg with a repeat dose and then increased dose to 6mg
-
DO NOT use in heart transplant recipient, wide complex tachycardia and WPW or previous allergy
- Dosing:
Wide Complex Tachycardia
Evaluation
- Is patient stable or unstable
- If unstable or in doubt call code blue and follow ACLS protocol
- If stable obtain EKG, troponin, and electrolyte panel including magnesium
- Look for precipitating cause and medication list for QT prolonging agents
Management
- Replete electrolytes
- Discontinue QT prolonged agents. Magnesium sulfate 2g IV should be given if patient have prolonged Qtc (>450 in women and >470 in men)
Hypotension
Evaluation
Decreased SVR: Exam = warm extremities, sometimes flushing
- Sepsis: common cause. Obtain blood culture x2, CXR, UA/micro/culture, and lactate. Rapid administration of IVF and antibiotic
- Medications: Look for antiHTN, pain meds, sedative, if concern for opioate overdose, give naloxone
- Adrenal insufficiency: Is the patient on chronic steroids and unable to mount a stress response? consider stress dose steroids
- Anaphylaxis: Give epinephrine 0.2-0.5ml SC/IM q20mins, benadyrl 50mg IV, hydrocortisone 100mg IV
Decreased preload: Exam= cold extremities
- Hypovolemia: STAT CBC, consider central venous pressure monitoring. Give IVF
- Pulm emboli
- Tension pneumothorax: Unequal breath sounds on examination. DO not wait for CXR. Insert 14 or 16 gauge needle into the second intercostal space at the midclavicular line ASAP
- Tamponade: elevated JVP, muffled heart sound and hypotension
- Right ventricular infact
- Pulmonary hypertension
Decreased contractility
- MI
- Medication
- Aortic dissection: Get STAT chest CT
Management
- Is the patient stable?
- Have low threshold to transfer a hypotensive patient to the ICU for better nursing support, pressors and/or intubation
- Treatment is aimed at the underlying cause but almost all cases call for fluid resuscitation. If suspicion of CHF is low then give rapid isotonic fluid resuscitation
- If there is concern for mixed cardiogenic and septic shock, let your volume exam guide treatment. Keep fluid boluses small (i.e 200ml and reassess). Trend lactate.
- In general, start O2, additional large bore peripheral IVs, put patient in trendelenburg, draw basic STAT labs (CBC, lytes, BUN, creatinine, glucose, LFTs blood/urine culture), STAT EKG, CXR, ABG/lactate
If the patient stable then ask this question
- Is this BP real?
- Is the BP different from prior values? if the patient usually has a BP 80/40 then the acuity may be decreased somewhat
- Is there associated hypoxemia, AMS, or increased RR (reasons for intubation)?
- Is the MAP <60? MAP less than 60 results in significant risk of hypoperfusion to vital organs
Hypertension
Evaluation
Physical examination
- Brain: headache, confusion, lethargy, stroke
- Eye: blurred vision
- Heart: Chest pain, dyspnea
- Kidney: low urine output, edema
Lab: not always required. Use selectively to determine cause and whether patient meets criteria for hypertensive emergency.
- CBC with peripheral smear
- EKG, troponin, BNP
- UA (looks for proteinuria), electrolytes, BUN and creatinine (look for renal dysfunction)
- CXR if chest pain or dyspnea
- Head CT for those with neurologic symptoms
- Chest CT with contrast in patients with severe chest pain, unequal BP in arms, unequal pulses, or widening of mediastinum on CXR
Management
For hypertensive urgencies: Majority of patient with HTN have no acute end organ damage and their BP can be lowered over days with oral medications. Consider rechecking BP after 30 minutes of quiet rest. Restarting a patient's home med is a good first step. Alternatively, consider starting one or more long acting oral med that can be continued on discharged.
- Amlodipine 5-10mg PO daily
- Lisinopril 10-20mg PO daily or losartan 25-50mg daily
In cases where more rapid lowering and closer tritration of BP is desired, consider shorter acting med
- Captopril 6.25-25mg PO TID
- Clonidine 0.1mg BID. can titrate to TID. DUe to the risk of rebound HTN, often reserved for resistant HTN
- Hydralazine 10mg PO q8hr can increase to q6hr. use with caution due to unpredictable effect and reflex tachycardia
For Hypertensive emergencies
- Labetalol: 10-20mg IV initial, followed by 10-80mg IV q10 mins until BP falls
- Nicardipine: Initial infusion of 5mg/hr, increasing by 2.5mg/hr every 5 mins to a maximum dose of 15mg/hr. Watch out for reflex tachycardia
- Nitroprusside: 0.3mcg/kg/min-4mcg/kg/min
- Esmolol: 0.5mg/kg loading dose, followed by starting infusion of 50mcg/kg/min up to 200mcg/kg/min
Fever
Differential
- Infection (lung, heart, brain, urine, sinuses, prostate, abdomen, skin, joints, lines, etc)
- Infammation (Collagen vascular disorder, neoplastic disorder)
- Mucositis
- Atelectasis
- Blood product reaction
- Drug fever (beta lactam antibiotics and amphotericin common causes)
- PE vs DVT
Is it a true temperature?
- Is it greater than >100.4 F?
- Quickly chart check and determine if patient is stable vs unstable (look at vitals, etc). If unstable go to bedside immediately!
If unstable:
First: Brief yet thorough chart check
Go assess bedside.
Get as much hx as you can - drug allergies, recent infections, blood transfusions, etc. Targeted exam (skin, lungs, extremities, etc). If patient is not responsive or sudden change in mentation, address those first.
- If you have an idea where the infection is coming from, start targeted antibiotics.
- If no idea where infection is coming from, repeat blood culture if > 48 hours since last blood culture. If blood culture performed less than 48 hours ago, usually no need to repeat blood culture.
-Consider pan culture - UA, Urine Clx, line clx, CXR, and EKG on top of repeat blood cultures.
- Labs to order (based on presentation/suspicion): CBC, CMP, Lactate, Trop, BNP, D-dimer, PT/PTT, etc.
- Also start broad-spectrum antibiotics (Vancomycin/Zosyn) (unless antibiotic allergies)
- ICU consult, Stat.
If stable:
- Assess where the nurse took temperature, is it in the correct location?
- Have RN recheck temperature in 30 mins and dochalo/ call you. You do not have to act on one temperature, first confirm it. (Exceptions might be if the patient is neutropenic, then consider neutropenic fever).
- Do a thorough chart check while you wait for a call back:
- Why was the patient admitted?
- What was the WBC?
- What was the urine output?
- Any recent meds/blood transfusions/surguries?
- If after 30 minutes temperature is confirmed, go assess patient bedside.
- Get a detailed history from patient.
- Do a thorough PE, looking for skin infections (including decubitus ulcers), and looking at all lines.
- If worried about an infectious cause, start appropriate antibiotics.
Low urine output
Normal urine output
- typically at least 0.5 cc/kg/hr.
- Oliguria: urine output < 400cc/day
- Anuria : urine output < 100cc/day
Do you believe the numbers?
- If patient has foley, flush tubing to make sure it is not clogged.
- If no foley, ask about urine output, look at daily weights, etc.
Examine patient bedside.
- Assess volume status: mucous membranes, skin pallor/dryness, edema, complaints of thirst, neck veins (assess CVP), crackles in lungs (pulmonary edema), bladder palpable on exam, prostate exam, etc.
Check a post-void residual by bladder scan.
- If volume > 300cc, then insert foley (In and out). If consistent > 300cc, keep foley in.
Causes of urinary retention:
- BPH, anticholiergic medication, side effect of medication:narcotics/benadryl/anestetics
Assess for renal failure (AKI)
- Prerenal, renal, postrenal causes.
- Look for fluid overload (CHF), and obstruction (renal US).
- If both negative, then fluid challenge is acceptable: 500cc L bolus. (Go to AKI for further management).
CHF/Volume overloaded? Initiate diuresis:
- Working kidneys: lower IVF rate and self-diuresis
- CHF/symptomatic: use lasix 20mg - 80mg IV
- Renal failure: Dialysis? If kidneys still working, can try high dose lasix - 160mg- 240mg IV Lasix.
Dyspnea
DDx (5 major categories of disease to consider)
Pulmonary
- Pneumonia = fever, purulent vs dry cough, pleuritic chest pain
- Pneumothorax = acute onset, pleuritic chest pain. Consider in any intubated patient.
- Pulmonary embolism = Hx DVT, recent surgery, pleuritic chest pain, tachypnea, tachycardia, hypoxia - Often difficult to rule in or out by history/exam. Consider this early.
- Aspiration = common problem if acute loss of consciousness
- Bronchospasm = seen with CHF, pneumonia, asthma/COPD
- Upper airway obstruction = often acute onset, stridor/focal wheezin- If albuterol fails, consider vocal cord dysfunction
- ARDS = usually in pts hospitalized with another dx (e.g. sepsis
Cardiac
- MI/ischemia = dyspnea can be an anginal equivalent
- CHF = common in elderly pts on IVF or due to ischemia
- Arrhythmia = can cause dyspnea with or without CHF/ischemia
- Tamponade = consider if signs of isolated right heart failure
Metabolic
- Acidosis = pts become tachypneic to blow off CO2 in compensation
- Sepsis = dyspnea can be an early, non-specific sign of systemic infection
Hematologic
- Anemia = easy to miss this by Hx/exam
- Methemoglobinemia = rare; consider if taking dapsone, nitrates, topical/local anesthetics
- - Cyanosis, blue discoloration of skin/mucous membranes confusion, seizures, normal PO2
Psychiatric
- Anxiety = common, diagnosis of exclusion
Evaluation of Patient
History
- Learn about acuity of onset of dyspnea
- Associated symptoms? (cough, chest pain, palpitations, fever)
- Review recent events or meds given at time of symptoms onset (IV fluids)
- Review relevant PMHx and admitting diagnosis
Physical exam
- Start by asking nurse for vital signs HR, RR, BP, O2 sat). Ask for second set 15-30 minutes later.
- Lung exam = listen for wheezes, rales, stridor, symmetry of breath sounds
- Cardiac exam = attention to JVP, carotids, rate/rhythm, murmurs/rubs
- Keep in mind adventitial lung sounds may be absent in someone with severe airflow limitation
- Look at extremities for edema (unilateral vs. bilateral) and perfusion (cool vs. warm, cap refill, cyanosis).
- Mental status = gives you idea of cerebral oxygen delivery
Labs/Studies
- EKG, CXR, ABG, CBC
- 4 basic studies will give you a good deal of information, and help you sort out what might be going on with your patient if it’s not clear from above.
- Consider CTPA if high risk of PE/DVT (Wells criteria)
Initial Management
A. Oxygen
- Initial intervention for any patient with dyspnea. Even CO2 retainers need O2 and it takes longer than the few minutes you need to evaluate them for significant respiratory depression to develop. Your goal is a PO2 > 60 or O2 sat > 92%. if nasal cannula isn't working (max FIO2 is ~40%), try a simple mask (up to 50%), non-rebreather (70%) or high humidity mask (90%). Remember that respiratory therapist (RT) is your friend; call early if you’re having any trouble and they will help with nebs, suction, masks, ABGs, oral/nasal airways
B. Diuretics
- Consider Lasix in any patient with history or exam consistent with CHF; other processes associated with increased lung water (pneumonia, ARDS).
- One dose of Lasix is unlikely to do any irreversible damage.
C. β-Agonists
- Bronchodilators will benefit patients with wheezing from any etiology
- Remember wheezing can occur in many conditions other than asthma (e.g., CHF, pneumonia)
D. Intubation
- Assess potential to protect airway (see Pulmonary section); consider calling ICU
E. Other
- Once you stabilized patient and results of initial studies returned, you can initiate directed therapy at the specific etiology of dyspnea.
Chest pain
I. DDx (Biggest killers)
- MI : Dull pressure pain associated with dyspnea, diaphoresis, radiation to left jaw/arm, N/V, cardiac risk factors present
- Aortic Dissection: Tearing pain that radiates straight to the back, associated with HTN, smoking Hx, unequal pulases
- Pneumothorax: Pleuritic chest pain, COPD, trauma, decreased breath sounds, hyperresonance, deviation of trachea away from affected side, hypoxia
- Consider in any intubated patient. - Pulmonary Embolism: Pleuritic chest pain, dyspnea, hypoxia, hemoptysis
- Other: Pericarditis, pneumonia/pleurisy, GERD, PUD, esophageal spasm, costochondritis, anxiety (diagnosis of exclusion), HOCM, myocarditis,
- If HIV/AIDS = herpes, CMV, candida esophagitis
Evaluation of Patient
History:
- Learn about acuity of onset of chest pain
- Associated symptoms? (cough, dyspnea, palpitations, fever)
- Review recent events or meds given at time of symptoms onset
- Review relevant PMHx and admitting diagnosis
- Look at initial EKG (from chart if available)
- Focus on ruling out the major killers rather than definite diagnosis
Physical exam:
- Start by asking nurse for vital signs (HR, RR, BP, O2 sat). Ask for second set 15-30 minutes later.
- Ask nurses to get immediate EKG as you walk to patient’s room.
- Lung/cardiac exam
Initial Labs/Studies to Order
- Ask nurses to get immediate EKG as you walk to patient’s room.
- Crisis panel
- CBC, CMP, troponin x3 q6h, CXR, ABG
- CHF = echo
Management
Suspected Angina/MI
- Start O2 by NC and give sublingual NTG 0.4mg q5 min x3; hold for SBP < 100
- Remember, if chest pain responds to NTG it does not automatically rule in angina.
- If ineffective, try other antianginals
- Metoprolol 5mg IV q5 min x 3 (avoid in COPD/asthma)
- Nitropaste
- If not already on aspirin/Plavix and has no contraindications, order ASA 325mg and Plavix 300mg x 1
- Further meds = high-dose statin, consider ACE inhibitors
Suspected Dissection
- Call and transfer to ICU to reduce BP and inotropy with beta-blocker
- Order CT scan or echo and call surgery
- EKG may show evidence of ischemia in RCA distribution if dissection is proximal
Suspected Pneumothorax
- Call surgery for chest tube placement
- If tension pneumothorax, immediate needle decompression at 2nd intercostal space at midclavicular line. Don’t wait for CXR.
Suspected PE
- ABG confirms hypoxia
- Consider CTPA or V/Q scan and start anticoagulation
Suspected Pericarditis
- NSAIDS and colchicine
Wrap up:
- Obtain post-pain EKG and document event
Combative or Confused patients
- Does the patient have altered mental status or is he/she upset over something?
- If there is any question of physical injury, call security (0). No matter how many years of commando training you have, it is not your responsibility to restrain patients in a safe manner. Also, patients generally tend to calm down when they are confronted by overwhelming numbers of people who are responsive to their needs or anxieties.
- Try to do as much of an altered mental status workup as you can. If you suspect an underlying reason for the agitation (pain, sundowning, hypoxia, medication), then obviously treat the underlying reason.
Management
Non-pharmacologic
- Accompaniment (sitter, family members at the bedside or via phone)
- Minimize restraint but if you
- If you feel restraints are needed, you need to put order under non-violent restraint specifying the type of restraint and the reason for initiating. They must be renewed every 24 hours. Generally, try to initiate the least restrictive type of restraint. Posey vests prevent patients from leaving the bed but leave the arms and legs free. Four-point cloth restraints limit the movement of arms and legs. They are more restrictive than Poseys but may be necessary if a patient is pulling out lines, etc.
Pharmacologic
- Haldol 0.5mg - 1mg BID PO or IM can also used as needed q4hr
- Quetiapine 12.5mg-25mg once at night
- Olanzapine 5mg-10mg IM, may repeat based on response 2 hrs after the initial dose and 4hrs after second dose. Max 30mg/day
- Benzo (avoid in elderly): 0.5-1mg q4hr
Falls
Evaluation/Management
- Assess patients at bedside. Look for any injury; any locality on exam must be worked up in the appropriate manner (e.g. head CT, plain films, immobilization, etc). In particular, look for: ecchymosis, abrasions, fractures, pain, asymmetry, deformity, decreased range of motion, look at head, hands, shoulders, hips, knees, feet.
- Do a complete neuro exam including gait, strength, and cerebellar tests. Mental status testing may be necessary if a patient is confused or altered.
- Check orthostatics.
- Try to find out the circumstances of the fall. Witnessed? By whom?
- Loss of consciousness (does the patient remember hitting the ground)? Mechanism (getting out of bed, going to bathroom, standing up, turning around, etc.)? Associated symptoms (premonitory aura, incontinence, dizziness, headache, visual symptoms, palpitations, chest pain, dyspnea)? Preceding actions (coughing, urinating, straining, standing suddenly)? Past medical history, prior falls)?
Differential diagnosis.
- Differentiate mechanical fall vs. transient loss of consciousness.
- Don’t forget the following:
- Neuro: seizure, CVA/TIA, gait disorder, Parkinson’s, vertigo, dementia, normal pressure hydrocephalus, poor proprioception
- Cardiac: arrhythmia, MI, vasovagal, hypovolemia, orthostasis
- Meds: new medication or new dose, especially sedative/hypnotics, antidepressants, antihypertensive, vasodilators, opioids, alcohol, diuretics (requiring frequent trips to the bathroom). Don’t forget alcohol and illicit drugs.
- Musculoskeletal: arthritis, pain, deconditioning, weakness
- Other: anemia, poor eyesight, dim lighting, room change, bed rails left down, wet floor. 4. Document the fall by writing a progress note.
Insomnia
- Trial non pharmacological measures first: sleep hygiene, noise reduction (ear plugs/muffs), reduce lighting, avoid night time interruptions if able, turn off TV/radio/etc. In room
- Before using pharmacotherapy, check patient allergies
- Melatonin is generally a safe starting point for medications, with 1-3mg PO scheduled at 9 to 10pm
- If not effective, can consider trazodone 50mg PO at bedtime (caution with orthostatic hypotension, atrial/ventricular arrhythmias)
- Can also consider benadryl 25-50mg or hydroxyzine 50-100mg PO nightly PRN (safer for elderly) insomnia. Watch for anticholinergic side effects (dry mouth, blurry vision, urinary retention) and use with caution if impaired cognition.
- If still ineffective can consider ambien 5-10mg PO nightly
- If above measures not effective, evaluate the patient before considering any strong sedatives.
Acid/Base And Electrolytes
Hyponatremia
Definition
- Mild: Serum Na 130-134mmol/L
- Moderate: Serum Na 120-129mmol/L
- Severe: Serum Na <120mmol/L
- Acute: <48hrs since development of hyponatremia
- Chronic: >48hrs since development of hyponatremia. (hyponatremia should be considered chronic whenever the duration is unknown.
Evaluation: Order serum osmolality, urine sodium, urine osmolality, TSH, Lipid panel.
Tips: Free water balance (Urine osmolality) is regulated by ADH. Sodium excretion (urine sodium) is regulated by aldosterone. If a patient has ESRD, the cause of hyponatremia is excess free water intake in the setting of impaired Kidney water excretion, and is not mediated by ADH.
Step 1: Differentiate from true hyponatremia from pseudohyponatremia.
- A normal or elevated effective serum osmolality (280mOsm/kg or greater) suggests pseudohyponatremia.
- Hypertonic states, like hyperglycemia or mannitol use, can cause hyponatermia by drawing water extracellularly and lowering serum sodium concentration. This is a true hyponatremia. Serum osmolality will be high, sodium should normalize with correction of hypertonic state.
- Correction formula for hyperglycemia: corrected Na = measured Na + [(serum glucose - 100)/100] x 1.6 . You can also use MD Calc
- Hyperlipidemia or increased protein can also cause a lab error that results in a falsely low sodium result.
Step 2: is ADH high or low? Compare serum osmolality to urine osmolality.
- If serum osm > urine osm, then ADH is low (kidneys are appropriately responding by maximizing water excretion). Causes are excess water intake or inadequate solute intake. A urine osm <100 also suggests normal free water excretion.
- If serum osm < urine osm, ADH is high. Proceed to step 3
- Check for iatrogenesis: are there high rates of hypotonic solution infusing?
- Look at what medications are mixed in (ex: IV abx in 500ml D5W 4x/day = 2L of free water).
- Check volume of free water flushes in patients getting tube feeds or other hypotonic oral intake.
- Consider primary polydipsia.
- Causes of inadequate solute intake: tea and toast diet (carbs and fats metabolize to water and CO2, so do not count as solutes), beer potomania (high beer intake relative to solute intake).
Step 3: If ADH is high, what is the volume status?
If ADH is activated, urine osmolality is usually >100. Urine Na can help to determine RAAS activation, which can narrow the differential in casese where volume status is not clear. A low urine Na (<20) suggests RAAS activation, as seen in hyper or hypovolemia; a high urine sodium may suggest SIADH.
Hypervolemic: DDx: CHF, nephrotic syndrome, liver failure.
- ADH is released in response to low effective arterial blood volume due to third spacing or poor perfusion.
- Urine Na will be low (<20) since the RAAS is activated in response to low arterial blood flow.
Hypovolemic:
- ADH is being released in response to low effective arterial blood flow due to fluid loss
- Extrarenal losses, like GI loss: urine Na will be low (<20) since aldosterone will also be activated
- Renal salt wasting: urine Na will be high (>20). Causes include salt-wasting nephropathy, adrenal insufficiency, cisplatin, thiazide diuretic use.
Euvolemic:
- Hypothyroidism: check TSH (The main mechanism for the development of hyponatremia in patients with chronic hypothyroidism is the decreased capacity of free water excretion due to elevated antidiuretic hormone levels)
- Glucocorticoid deficiency: check AM cortisol
- SIADH: Inappropriate release of ADH independent of effective arterial blood flow. Urine Na will be high, since aldosterone is low.
- SIADH is a diagnosis of exclusion with following features:
- Clinical euvolemia
- Normal thyroid and adrenal function, no recent diuretic use
- Lab findings: Urine osmolality >150mOsm, serum osm <275 mOsm, Urine Na >20 mmol/L with normal dietary salt intake.
Management: Repeat BMP q4hr. Goal to increase Na no more than 4 to 6 mEq/L in 24hrs to prevent osmotic demylination syndrome. Start treatment based on volume status
Evaluate and treat severe symptoms emergently in all patients
-
The presence of these signs suggests cerebral edema and required rapid treatments: visual changes, neurologic deficits, encephalopathy, coma, respiratory arrest, and seizures.
-
Start on hypertonic 3% saline immediately at rate 15 to 30mL/hr and consult nephrology. Monitor serum sodium hourly while on hypertonic saline. If sodium is correcting too fast, stop hypertonic saline and start on D5W infusion.
Select treatment approach based on volume status, severity, and etiology.
Hypovolemia:
- Start on IV fluids Normal saline @100mL/hr. Caution: once volume status is corrected, a brisk aquaresis may ensue and cause overcorrection, thus, strict urine output and frequent sodium monitoring is critical. The earliest and most concerning indication of overcorrection is brisk urine output and/or a decrease in urine osmolality.
SIADH:
- Treatment of underlying cause/withdrawal of causative agents as possible.
- Start with fluid restriction 1-1.5L/day but restriction alone is often inadequate. Do not restrict beyond 1L, as that is unlikely to add additional benefit and can cause significant discomfort.
- Use urine electrolytes (Urine sodium + Urine potassium) to guide therapy:
- UNa + UK < serum Na: Positive free water clearance. Patient is still urinating out free water but not enough to improve hyponatremia. This suggests fluid restriction will be an effective treatment.
- UNa + UK > serum Na: Negative free water clearance. All free water is reabsorbed and any urination will continue to lower serum Na. This suggests osmole supplementation (hypertonic saline or salt tabs) is needed to treat hyponatremia.
- Any IV fluids with Na content less than UNa + UK will result in worsening hyponatremia because the kidney is able to excrete the solute but reabsorb the free water from the infused solution. Therefore, UNa + UK >154 is typically an indication that hypertonic saline is needed to correct hyponatremia.
- Additional therapies for SIADH:
- Hypertonic saline: Effective (3% = 513mEq/L), necessary when UNa+UK is very high. Requires good venous access. Not a long term therapy.
- NaCl tabs: 1g NaCl tab = 17mEq Na and 17 mEq Cl. Not a very high osm load per tab (typically need upwards of 2g TID). Difficulty pill burden, can stimulate thirst counteracting fluid restriction and cause GI upset.
Hypervolemia:
- Free water restriction (1-1.5L.day)
- Loop diuretics to optimize volume status
- Hypertonic saline and salt tabs generally NOT recommended as they will worsen volume overload.
If the serum sodium has been overcorrected:
- IV D5W
- Can give 3mL/kg/hr D5W to lower [Na] by approximately 1mEq/L/hr if overcorrected
- Pay attention to ongoing losses: if urine output is brisk (>150mL/hr) and dilute, the patient is losing free water rapidly and it is raising serum Na rapidly. Suggest nephro consultation to assist with safe correction strategies (eg: titrating D5W drip to a % of urine output or using DDAVP to inhibit the aquaresis)
Diagnosis and Management of disorders of body tonicity-Hyponatermia and Hypernatremia
Clinical practice guideline on diagnosis and treatment of hyponatremia
Hypernatremia
Definition:
- Serum Na >135 mmol/L. Chronic means > 48 hours. Acute means < 48hrs.
Etiology:
Renal water loss (U osm <700-800)
- loop diuretics
- Osmotic diuresis (hyperglycemia, mannitol, urea)
- Diabetes Insipidus: Central (trauma/post-surgical, pituitary lesions, sheehan's syndrome) vs Nephrogenic (congenital, sickle cell, hypercalcemia, severe hypokalemia, drugs: lithium, amphotericin)
Extra-renal water loss (U osm >700-800)
- GI loss: vomiting, NGT, osmotic diarrhea, lactulose, malabsoption
- Insensible loss: fever, burns, exercise
- hypertonic intake: hypertonic saline, excess salt intake, hypertonic sodium bicarb pushes
Evaluation: U osm, U Na, volume status
- Causes is often apparent from history and review of medications, nutrition, and intake/output
- Determine if there is inappropriate renal free water loss
- In DI, urine will be inappropriately dilute (<300 mOsm/L). Water deprivation test will result in rising serum Na and persistently dilute urine. Desmopression response after deprivation can differentiate nephrogenic (no response) vs central (concentrated urine)
Management
Step 1: calculate free water deficit. Can also use MD Calc

- % body water for 0.6 for male and 0.5 for female. If elderly use 0.5 for male and 0.45 for female
- Give free water deficit enterally
- Do not forget to correct Na if hyperglycemia also present

Step 2: Rate of correction
- Divide free water deficit by 24hrs and give accordingly. Check serum Na every 6-12hrs to adjust correction rate and follow urine output
- Rate of correction depends on acuity of onset and risk:
- chronic (>48hrs): 12 mEq/d appears safe w/o risk of cerebral edema
- acute (<48hrs): may decrease Na by 2 mEq/L/h until Na 145
- hyperacute (min-hrs) & life threatening (ICH, seizure): rapidly infuse D5W plus minus emergent HD
Diagnosis and Management of Disorders of Body Tonicity-Hyponatremia and Hypernatremia
Rate of correcting of hypernatremia
Hypokalemia
Definition:
- Serum <3.5mmol/L
Etiology:
- Intracellular shifts: Hypothermia, Exogenous insulin/refeeding, beta-agonists
- GI Potassium loss
- Metabolic acidosis: diarrhea, laxative abuse
- Metabolic alkalosis: Vomiting, NGT
- Renal Potassium Losses
- Hypotensive or normotensive
- Metabolic Acidosis: DKA, RTA type I and II
- Metabolic Alkalosis: diuretic (thiazide > loop)
- Drugs: amphotericin, cisplastin
- Hypomagnesemia
- Hypertensive: Mineralcorticoid excess
- Hypotensive or normotensive
Evaluation:
Review medication list
Order basic labs: Serum BMP, Mg, Serum osmolality, urine electrolytes (Na, K, Cl), Urine osmolality
Distinguish renal from GI losses with urine potassium.
- Urine K/Cr >13 mEq: Renal loss ; Urine K/Cr <13mEq: extrarenal loss
- If inappropriately high urine potassium excretion, consider sending plasma renin activity and aldosterone level
- High renin: suggests diuretics, GI losses, renovascular disease
- Low renin and high aldosterone: primary aldosteronism
- Low renin and low aldosterone: non-aldosterone mineralcorticoid excess such as licorice ingestion
Severe hypokalemia, get an EKG. Changes include U wave, inverted T wave, ST depression, PR and QRS prolongation and can lead to Vfib.
Management: There is a replacement protocol that can be ordered. So the RN can replaced it based on the hospital protocol.
- Replete magnesium first if low
- Replete potassium to >3 or >4 if high risk (HTN, CHF, arrythymia, MI, cirrhosis)
- Supplementation can be given Oral or IV. Oral potassium replacement is first choice. Caution in patient with peptic ulcer disease. Higher doses can cause stomach upset.
- Suggested potassium replacement doses.
- Serum K: 3.7-3.8: 20 mEq KCl IV or PO
- Serum K: 3.5-3.6: 40 mEq KCl IV or PO
- Serum K: 3.3-3.4: 60 mEq KCl IV or PO
- Serum K: 3.1-3.2: 80 mEq KCl IV or PO
- Serum K: less than equal 3.0: 100mEq KCl IV or PO
Caution in renal failure or ESRD. Always check the creatinine prior to replacing potassium. Give about half the suggested dose of potassium in patient with decreased GFR
Disorders of potassium homeostasis. Hypokalemia and hyperkalemia
Hyperkalemia
Definition
- Serum K+ >5.3-5.5
Etiology:
- Pseudohyperkalemia- K release from cells after blood draw, IVF with K
- Impaired excretion
- Low GFR (AKI or CKD)
- Drugs (spironolactone, ACEi, ARB, TMP-SMX, NSAIDs, digitalis overdose, heparin, chemo therapeutic agents)
- Shift from intracellular to extracellular compartment
- Excessive K intake
- Hemolysis
- Marked thrombocytosis or leukocytosis
- Ingestion (K Supplements, dietary salt substitutes)
- Iatrogenic
- Low mineralocorticoid state (adrenal insufficiency, type IV RTA)
- Acidosis
- Insulin deficiency or resistance including DKA
- Cell death (rhabdomyolysis, burns, tumor lysis)
- Retroperitoneal hemorrhage
- Old (hemolyzed) pRBC transfusion
Clinical manifestations:
- Weakness, nausea, paresthesia, palpitations
Evaluation:
- Repeat serum K+ and assess renal function studies including serum Cr and BUN
- Order stat ECG to evaluate for hyperkalemia related changes (Tall peaked “tented” T waves, PR interval prolongation followed by loss of P waves, QRS widening, sinus wave pattern, VF/asystole/PEA
- Review medications for offending drugs and stop as appropriate/indicated
Management: PowerChart “Hyperkalemia (TH) Protocol”
Approach to Rx:
-
Order ECG for serum K >5.5 and treat emergently if ECG changes noted. Rx any K >6.5 emergently regardless of ECG changes
-
Repeat ECG every 30-60 mins to ensure resolution of ECG abnormalities and consider telemetry for monitoring.
-
Check and treat concurrent electrolyte abnormalities as they increase risk for arrythmias
-
Check if sample is hemolyzed and repeat serum K measurement to verify
Treatment aims:
- Stabilize the myocardial membrane
- Temporarily shift K into cells
- Eliminate K from body
Cardiac membrane stabilization:
- Calcium chloride 0.5-1g IV (more potent, but must be given via central line)
- Calcium gluconate 1-2g IV
- No effect on serum K level. Should normalize ECG. If not, re-dose.
Temporarily shift K into cells:
- Regular Insulin 10 units IV + D50 100ml IV. If high risk for hypoglycemia, monitor blood glucose closely. If hyperglycemic, insulin can be given alone.
- Beta2-agonists (albuterol 10-20mg in 4mL saline nebulized)
- NaHCO3 50-100 mEq
Eliminate K from body:
- Preferably renal elimination
- IVF with NS or NaHCO3- First line in hypovolemic patients
- Loop diuretic: Furosemide 40-160 mg IV- First line in hypervolemic patients and given with IVF if euvolemic
- Thiazide diuretic: Adjunct use with loop diuretic may be useful
- GI cation exchangers- Exchange Na+ for K+ in the GI tract
- Sodium zirconium cyclosilicate (Lokelma)- 10 g TiD for up to 48hr, then 5-15g q.other daily-daily as maintenance
- Kayexalate (sodium polystyrene sulfonate)- 15-30 g PO (slow onset and controversial use; associated with bowel necrosis and contraindicated in post-op patients and those with risk of/obstruction
- Dialysis-can be used in patients with acute/chronic renal failure who fail medical management; improves serum K relatively quickly but lengthy process to initiate therapy (nephrology consult, machine and catheter placement)
- Continues renal replacement therapy-slow correction and requires ICU setting
Key Points:
-
Hyperkalemia protocol can be initiated/ordered from PowerChart
-
Serum K level >6.5 or hyperkalemia with ECG changes warrant emergent treatment with calcium gluconate or CaCl
-
Strategy to shift K into cells is useful acutely as it works fast but is only a temporary measure and it should be accompanied by therapies to eliminate K from the body
-
K elimination renally is most efficient and takes into consideration patient’s volume status
Hypomagnesemia
- Serum Mg++ <1.8 mg/dL
Etiology:
- Malnutrition (assc. with heavy chronic alcohol use causing renal wasting)
- Malabsorption or diarrhea/GI loss
- PPI induced
- Renal losses (polyuria and high tubular flow, e.g., osmotic diuresis, post-ATN diuresis)
- Hypercalcemia (e.g. hyperparathyroidism)
- Loop and thiazide diuretic associated
- Proximal tubular toxins (e.g. aminoglycosides, amphotericin, cisplatin)
- Calcineurin inhibitors (tacrolimus > cyclosporine)
- Volume expansion (reduced Mg++ reabsorption due to reduced Na and H2O reabsorption)
- Gitleman and Bartter syndromes
- Uncontrolled DM, post-parathyroidectomy (Hungry bone syndrome)
Clinical manifestations:
- NM hyperexcitability (tremor, tetany, convulsions), weakness, delirium, coma
- CV (widening QRS, peaked T waves, wide PR interval, atrial and ventricular arrhythmias)
- Hypocalcemia, hypoparathyroidism, PTH resistance, and decreased calcitriol synthesis
Evaluation:
- Order CMP, serum Mg++ and Phosphorus level
- Review patient history, clinical circumstances, nutritional status and medications
Management: PowerChart “Electrolyte Replacement Protocol”
Approach to Rx:
Route and dose based on severity of clinical manifestations and degree of hypomagnesemia
Patients with no or minimal symptoms:
- PO repletion recommended if able to tolerate
- Can give IV if unable or have GI side effects (discomfort, diarrhea)
- Typical daily PO dose in patients with normal renal function is 240-1000mg (20-40 mEq of elemental Mg++ in divided doses
Patients with severe symptoms: tetany, arrhythmias, seizure
- 1-2 grams (8-16 mEq) Magnesium sulfate bolus over 2-15mins if hemodynamically unstable (including those with arrhythmias consistent with torsade de pointes or hypomagnesemic hypokalemia). Repeat bolus if remains hemodynamically unstable
- If hemodynamically stable, give 1-2 grams Magnesium sulfate in 50-100mL of D5W over 5-60mins followed by infusion of 4-8 grams MgSulfate slowly over 12-24 hrs
- Adjust dose in AKI and CKD due to risk for severe hypermagnesemia
- Measure serum Mg 6-12 hrs after each IV dose and adjust dose accordingly
For routine IV or maintenance repletion, use the following estimated repletion doses:
- If the plasma Mg++ is < 1 mg/dL, give 4 to 8 grams (32 to 64 mEq of magnesium sulfate over 12 to 24 hours and repeat as needed.
- If the plasma Mg++ is 1 to 1.5 mg/dL, give 2 to 4 grams (16 to 32 mEq of magnesium sulfate over 4 to 12 hours.
- If the plasma Mg++ is 1.6 to 1.9 mg/dL, give 1 to 2 grams (8 to 16 mEq of magnesium sulfate over 1 to 2 hours.
(Conversion relationships: 1 mmol = 2 mEq = 24 mg of elemental magnesium = 240 mg magnesium sulfate.)
Key Points:
- Correct the underlying disease
- Correct Mg++ based on severity of hypomagnesemia and symptoms if any
- Great caution should be exercised when treating hypomagnesemia in AKI and CKD patients due to the increased risk for severe hypermagnesemia
- Replacement therapy with IV magnesium in patients with arrhythmias or NM symptoms
Hypermagnesemia
Definition
- Serum Mg++ >2.3 mg/dL
Etiology:
- Insufficient excretion due to CKD
- Iatrogenic/excess intake due to overaggressive replacement, Magnesium-based laxatives/enemas use in CKD, Mg++ administration during preeclampsia/eclampsia treatment
Clinical manifestations:
Symptoms are either cardiovascular vs neuromuscular manifestations or hypocalcemia
- Plasma Mg++8-7.2mg/dL: Nausea, flushing, headache, lethargy, drowsiness and hyporeflexia
- Plasma Mg++2-12mg/dL: Somnolence, hypocalcemia, areflexia, hypotension, bradycardia and ECG changes
- Plasma Mg++ >12: Muscle paralysis leading to flaccid quadriplegia, apnea/respiratory failure, complete heart block, cardiac arrest
Evaluation:
- Order CMP, serum Mg++
- Review patient history, clinical circumstances and medications
Management:
Treatment is tailored based on severity and clinical manifestations and renal function
- Asymptomatic patients: Cessation of Mg++ supplementation therapies
- Symptomatic patients: 1gram Calcium Gluconate IV over 10mins to antagonize Mg++
- Moderate renal impairment (eGFR 15-45): Consider IV Isotonic fluid plus loop diuretic (e.g., Furosemide)
- Severe renal impairment (eGFR <15)/Symptomatic patients: Dialysis is the definitive therapy
Key Points:
- Clinically relevant hypermagnesemia is rare and is usually due to excessive magnesium administration in patients with CKD or impaired magnesium excretion
- Severe hypermagnesemia may need dialysis
Hypocalcemia
Evaluation:
- verify with repeat measurement that there is a true decrease in the serum calcium concentration (total serum calcium corrected for albumin or ionized calcium)
- Note alkalosis augments calcium binding to albumin and increases severity of symptoms
- Compare with previous values if available
- If the patient has a low albumin-corrected serum calcium or ionized calcium concentration, further evaluation to identify the cause is indicated
- Obtain thorough history and physical examination.
- measure serum intact parathyroid hormone (PTH)
- Other measurements that may be helpful include serum magnesium, creatinine, phosphate, vitamin D metabolites (primarily 25-hydroxyvitamin D [25(OH)D]), and alkaline phosphatase.
Causes:
- renal failure
- hypoparathyroidism or pseudohypoparathyroidism (PTH resistance)
- severe hypomagnesemia or hypermagnesemia
- acute pancreatitis
- rhabdomyolysis
- tumor lysis syndrome
- vitamin D deficiency
Signs:
- paresthesias, tetany (especially carpopedal spasm), lethargy, confusion, seizures,
Trousseau's sign, Chvostek's sign, decreased cardiac function, QT prolongation
Treatment:
- Symptomatic hypocalcemia ( see symptoms above) or asymptomatic hypocalcemia with an acute decrease in serum corrected calcium to ≤7.5 mg/dL (≤1.9 mmol/L) or ionized calcium to ≤3 mg/dL (≤0.8 mmol/L) should be corrected by replacement with calcium gluconate IV.
- 1 or 2 g of calcium gluconate, equivalent to 90 or 180 mg elemental calcium, in 50 mL of 5% dextrose or normal saline) can be infused over 10 to 20 minutes
- If present, low Mg should also be corrected because it contributes to low Ca.
For those with milder symptoms of neuromuscular irritability (paresthesias) and corrected serum calcium concentrations greater than 7.5 mg/dL (1.9 mmol/L) or a serum ionized calcium concentration greater than 3.0 mg/dL (0.8 mmol/L), initial treatment with oral calcium supplementation is sufficient. If symptoms do not improve with oral supplementation, IV calcium infusion is required.
Hypercalcemia
Evaluation:
- verify with repeat measurement that there is a true increase in the serum calcium concentration (total calcium corrected for albumin or ionized calcium)
- Compare with previous values if available
- Clinical evaluation, including duration of hypercalcemia, presence or absence of symptoms, family history, and medications, may help determine the etiology of hypercalcemia
Causes:
- primary hyperparathyroidism
- malignancy (PTH related peptide, ectopic production of 1,25, dihydroxyvitamin D, osteoclast activating factor
- lytic bone mets
- non parathyroid endocrine disorder
- thyrotoxicosis, pheochromocytoma, adrenal insufficiency, VIP-producing tumor
- granulomatous disease (1,25 dihydroxyvitamin D excess)
- sarcoidosis, tuberculosis, histoplasmosis, coccidiomycosis, leprosy
- medications (thiazide diuretics, lithium, estrogens, antiestrogens)
- milk-alkali syndrome
- vitamin A or D intoxication
- familial hypocalciuric hypercalcemia
- immobilization
- parenteral nutrition
- acute and chronic renal failure
Signs:
- "Stones, moans, groans, with psychic overtones*.
- Renal: polyuria (nephrogenic DI), nephrolithiasis, renal failure, ectopic calcification
- Gl: anorexia, nausea, vomiting, constipation
- Neuro: weakness, fatigue, confusion, stupor, coma
- ECG: Shortened QT
Treatment:
- avoid factors that can aggravate hypercalcemia, including thiazide diuretics and lithium carbonate therapy, volume depletion, prolonged bed rest or inactivity, calcium and/or vitamin D supplements, and a high-calcium diet (>1000 mg/day)
- Mild hypercalcemia - asymptomatic or mildly symptomatic with with serum calcium level of 12 and 14 mg/dL [3 to 3.5 mmol/L]) may not require immediate therapy
- Moderate hypercalcemia - Asymptomatic or mildly symptomatic individuals with chronic moderate hypercalcemia (calcium between 12 and 14 mg/dL [3 to 3.5 mmol/L]) may not require immediate therapy
- Severe hypercalcemia - serum calcium levels of >14 mg/dL [3.5 mmol/L]) or symptomatic (eg, lethargy, stupor) require aggressive therapy.
- → Initial therapy of severe hypercalcemia includes the simultaneous administration of intravenous (IV) isotonic saline, subcutaneous calcitonin, and a bisphosphonate (typically, IV zoledronic acid)
- Correct dehydration, increase renal calcium excretion, decrease bone resorption, and treat the underlying disorder.
- IV hydration, initial rate is 200 to 300 mL/hour that is then adjusted to maintain the urine output at 100 to 150 mL/hour
- In individuals with renal insufficiency or heart failure, careful monitoring and judicious use of loop diuretics (after intravascular volume has been repleted) may be required to prevent fluid overload. IV furosemide
- Specific treatment in approximate desirability of use:
- For immediate, short-term management in severe hypercalcemia (Ca >14 mg/dl) and symptomatic patients (lethargy, stupor), administer Calcitonin in combination with NS hydration and Bisphosphonates. Initial Calcitonin dose is 4 units/kg, administered SQ or IM. Repeat serum calcium in 4-6 hrs. If lowering of calcium levels is noted, continue 4 U/kg BID for 24-48 hrs. May increase to 8 U/kg Q12H or Q6H for 24-48 hrs if response is not satisfactory with 4 U/kg BID.
- Among IV bisphosphonates, Zaldronic Acidis preferred over pamidronate (60 to 90 mg over 2 hours) because it is superior to pamidronate in reversing hypercalcemia related to malignancy. The initial dose is 4 mg IV over 15 minutes.
- Pamidronate 15-45 mg IV as single IV infusion or 90 mg over 2-24 hours would be another option for treatment
https://www.uptodate.com/contents/treatment-of-hypercalcemia?search=hypercalcemia&source=search_result&selectedTitle=2~150&usage_type=default&display_rank=2
Hypophosphatemia
Evaluation:
- Serum phosphorus levels should be interpreted with concomitant evaluations of PTH, serum total and ionized calcium, urine phosphate and calcium and Vitamin D
- Medical history, physical examination and lab tests to determine etiology of hypophosphatemia (renal wasting, decreased intestinal absorption etc)
- Concomitant serum levels of Magnesium and Potassium should be checked as well and replaced per protocol
Causes:
- Hyperparathyroidism
- Vitamin D deficiency
- Malabsorption/emesis
- Increased urinary secretion
- Refeeding after malnutrition
- Hyperalimentation
- Recovery of DKA, effects of insulin/glucagon/androgens
- Hypothermia (recovering from hypothermia)
- Steatorrhea
- Medication (e.g. phosphate binders, salicylate poisoning, steroids, diuretics)
- Decreased intake
- Alcohol abuse, withdrawal
- Renal tubular defects (aldosteronism, SIADH)
- Sepsis
- Gout
- Burns
- Respiratory alkalosis
- Hypomagnesemia
Signs: Generally seen with serum phosphate levels below 1 mg/dl
- Numbness
- Weakness
- AMS / confusion
- stupor
- Seizures
- coma
- Muscle pain
- Rhabdomyolysis
- Resp. failure
- CHF
- Paresthesias
- Dysarthria
- Hemolysis
- Platelet dysfunction
- Metabolic acidosis
Therapy:
- Treat underlying cause, the phos levels will normalize automatically ( DKA, diarrhea, chronic antacid therapy, or vitamin D deficiency)
- Replete if serum phos levels are less than 2.0 mg/dl (0.64 mmol/L)
- Keep phos levels over 1 mg/dl, above that, oral replacement is preferable to avoid hyperphosphatemia ( which can cause subsequent hypocalcemia, ectopic calcifications, renal failure, or hypotension)
- In Asymptomatic patients with serum levels below 2.0 mg/dl replete with oral phosphate
- Serum level of 1.5 mg/dl (0.48 mmol/L) → give 1 mmol/kg elemental phosphorus (minimum of 40 and maximum of 80 mmol can be given in 4 doses over 24h)
- Serum level less than 1.5 mg/dl → give 1.3 to 1.4 mmol/kg of elemental phosphorus (up to a maximum of 100 mmol given in 4 doses over 24h)
- In Symptomatic patients treatment varies with severity of the hypophosphatemia
- Serum level of 1.0 to 1.9 mg/dl (0.32 to 0.63 mmol/L) → treat with oral phosphate
- Serum level less than 1.0 mg/dl → treat with IV phosphate and switch to oral
- Stop replacement when serum levels is equal to or greater than 2.0 mg/dl
- IV preparations: IV phosphate is potentially dangerous. If IV phos is necessary, use dose depending on severity of hypophosphatemia and the weight of the patient.
- If the serum phosphate concentration is greater than or equal to 1.25 (0.40 mmol/L), → give 0.08 to 0.24 mmol/kg over six hours (up to a maximum total dose of 30 mmol).
- If the serum phosphate concentration is less than 1.25 mg/dL (0.40 mmol/L) → give 0.25 to 0.50 mmol/kg over 8 to 12 hours (up to a maximum total dose of 80 mmol).
→ measure serum phosphate levels Q6H and switch the oral replacement once serum levels have reached 1.5 mg/dl (0.48 mmol/L)
- Use either sodium phosphate or potassium phosphate depending on whether patient also needs potassium
- Follow Potassium and Magnesium as well and replete per protocol
https://www.uptodate.com/contents/hypophosphatemia-evaluation-and-treatment?search=hypophosphatemia&source=search_result&selectedTitle=1~150&usage_type=default&display_rank=1#H727383
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4324571/#:~:text=When%20evaluating%20a%20patient%20with,not%20reliable%20indicators%20of%20total
Hyperphosphatemia
Definition
- Serum Phosphate >4.5mg/dL.
Etiology/Risk Factors
- Increased intake (external/internal):
- Excessive vitamin D (increases GI absorption of PO4) or vitamin A.
- Phosphate-containing enema, particularly in patients with kidney insufficiency.
- PO4 replacement.
- TPN (through administration of excess phosphate).
- Excessive dietary phosphate in patients with advanced CKD (usually Stage >4).
- Shifts from cells into serum:
- Acidosis (lactic acidosis, DKA).
- Hypoinsulinemia.
- Rhabdomyolysis.
- Tumor lysis.
- Decreased excretion/increased reabsorption:
- Bisphosphonates.
- Decreased PTH secretion or renal resistance to PTH (hyper- or hypomagnesemia).
- Kidney disease (GFR <30).
- Often accompanied by hypocalcemia due to calcium-phosphorus complex formation.
Evaluation
Laboratory tests to order:
- CMP.
- Calculate a calcium-phosphate product ([Calcium] x [Phosphate]).
- At risk for calciphylaxis, renal osteodystrophy, and ectopic calcification if product > 55.
- LDH, uric acid if clinical concern for tumor lysis syndrome.
- CK if clinical concern for rhabdomyolysis.
Management
- ACUTE: rhabdomyolysis, tumor lysis, exogenous phosphate load.
- If acute process and developing renal failure or symptomatic (with severe hypocalcemia), may require hemodialysis.
- If kidney function is preserved, most causes of hyperphosphatemia will resolve by addressing the underlying cause (stopping vitamin D, resolution of tumor lysis, etc.). IV fluids may be given to facilitate phosphate excretion.
- CHRONIC: chronic kidney disease and secondary hyperparathyroidism.
- Low phosphate diet and phosphate binders as necessary (sevelamer, calcium acetate, lanthanum carbonate, etc.). Dialysis removes phosphorus, but given that only a small fraction of phosphorus is in plasma, there is significant rebound post-HD, hence the need for adjunctive therapies.
Key Points
- If kidney function is preserved, most other causes of hyperphosphatemia will resolve by addressing the underlying cause.
- Consider hemodialysis for acute, severe hyperphosphatemia complicated by symptomatic hypocalcemia and AKI/CKD.
- Hemodialysis (3x/week) is not typically effective for chronic hyperphosphatemia, and most patients with ESRD will require low phosphate diet and phosphate binder therapy.
- Calculate calcium-phosphate product to determine risk for complications.
Algorithm For Acid Base Disorders
Before You Begin: Gather Data
What lab tests do you need?
- ABG vs. VBG
- VBG can provide reliable estimation for pH (0.02-0.04 lower than ABG) and HCO3 (1-2 mEq higher than ABG).
- pCO2 on VBG is higher than arterial PaO2 by 4-9mmHg.
- ABG is necessary to accurately assess PaCO2 in hypercapnia or severe shock.
- BMP.
- Albumin.
Step 1: Determine Primary Acid-Base Disturbance.
- Remember that chronic acid-base disturbance(s) and/or mixed acute acid-base disturbances can be obscured by a normal pH.
- Consider the following “normal” values:
• Arterial pH: 7.40
• Arterial pCO2: 40
• Bicarb (HCO3): 24
• Anion gap: 12 - Acidemia
• pH < 7.38
• Primary disturbance
• Respiratory acidosis = pCO2 > 42
• Metabolic acidosis = HCO3 < 22 - Alkalemia
• pH > 7.42
• Primary disturbance
• Respiratory alkalosis = pCO2 < 38
• Metabolic alkalosis = HCO3 > 26
Step 2a: Calculate and Interpret the Anion Gap
- Anion gap (AG) = [Na] – [Cl] – [HCO3].
- Normal AG = 8-12 mEq/L with a serum albumin of 4g/dl.
- The normal AG depends on serum albumin. The expected "normal" range for AG can be calculated by 2.5 x albumin (g/dl) +/- 2.
- For severe hypoalbuminemia (2.0 g/dl), the expected gap would be 5 +/- 2, and an AG of 8-12 would be abnormally elevated.
- Paraproteinemia (especially polyclonal or monoclonal IgG) can lower anion gap due to the abundance of cations added to the system; this should be accounted for when evaluating anion gap since it could obscure a truly elevated AG.
- For calculation, >12 is generally used as the cutoff for a high AG. Because 12 is the upper limit of normal, keep in mind that approach might increase specificity for elevated AG at the cost of sensitivity. Because of person-to-person variation in “normal” AG, it can be useful to review a patient’s previous values of AG to establish a baseline and give context to small, acute changes in AG.
- If the AG is elevated, there is an anion gap metabolic acidosis present. Proceed to step 2b.
- If the AG not elevated, there is not an anion gap metabolic acidosis present. Proceed to step 3.
Step 2b: Calculate and Interpret the Excess Anion Gap
- If there is an anion gap, determine whether the excess in AG fully explains the drop in bicarbonate.
- For every 1 unit increase in AG (△AG↑) from its upper limit of normal value (12), there is an expected 1 drop in HCO3 (△HCO3↓) from its “normal” value (24).
- If the AG and HCO3 are balanced, (△HCO3 ± 5mmol/L ≈ △AG), there is no concurrent metabolic process.
- If the HCO3 is lower than expected (△HCO3 ± 5mmol/L > △AG), there is a concurrent non-elevated anion gap metabolic acidosis as evidenced by a reduction of HCO3.
- If the HCO3 is higher than expected (△HCO3 ± 5mmol/L < △AG), there is a concurrent metabolic alkalosis as evidenced by an excess of HCO3.
- The 5mmol/L correction accounts for the normal range of bicarbonate.
- Alternate approach to answer this question: “correcting” the bicarb.
- Corrected HCO3 = HCO3 + (AG - 12).
- If the sum is greater than the usual bicarbonate range (> 28), there is a concomitant metabolic alkalosis. If the sum is less than the usual bicarbonate range (< 22), there is a concomitant non-elevated anion gap metabolic acidosis.
- Finally, there is a third approach to this same problem, “the delta-delta,” which is not discussed here.
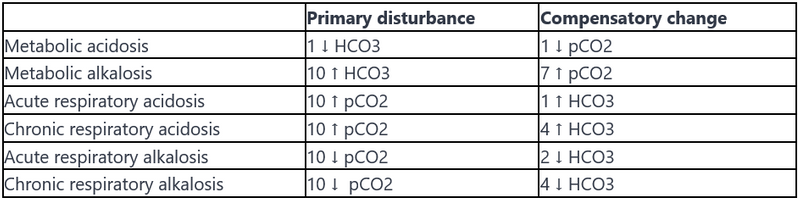
Step 3: Evaluate for Compensation
Evaluate for physiologic compensation for the acid-base disorder.
Any values above or below expected suggest an additional acid-base disturbance; a compensation should not normalize or overcorrect the pH.
The following table gives a quick rule-of-thumb for evaluating compensation. More detailed formulas are listed below.
Common Questions in Metabolic Acidosis
-
What is the pathophysiology of saline-induced normal anion gap (hyperchloremic) metabolic acidosis?The normal anion gap metabolic acidosis resulting from large volume administration of normal saline (NS) can be explained as a dilutional effect on the existing bicarbonate level. This is because NS contains a supraphysiologic concentration of chloride (154 mEq/L) and no bicarbonate; thus it will raise serum chloride while diluting other anions - namely lowering bicarbonate - inducing a metabolic acidosis. This may be avoided by using a balanced intravenous solution such as Lactated Ringer’s or Plasmalyte. These solutions have a lower [Cl-] concentration compared to NS and, most importantly, contain lactate and acetate respectively, which are rapidly metabolized to an equimolar amount of bicarbonate.
-
What are the disadvantages of giving bicarbonate in the setting of acute metabolic acidosis?
-
Can cause an initial transient worsening of intracellular acidosis.
-
Can lead to generation of increased CO2 which causes respiratory acidosis (especially in patients with respiratory failure such as in ARDS).
-
Can represent a large sodium load that can exacerbate hypervolemia.
-
Can worsen hypokalemia.
-
-
The 2008 Surviving Sepsis guidelines recommend against its use in sepsis if pH > 7.15. One can consider temporary NaHCO3 administration in the setting of severe metabolic acidosis (pH < 7.1) or to facilitate permissive hypercarbia. In most cases of normal anion gap metabolic acidosis, it is probably safe. Consider renal replacement therapy in cases of severe acidosis refractory to medical therapy.
Key Points
- It is important to follow a systematic approach each time interpreting a blood gas. Establish the primary disorder. Calculate AG to reveal an anion gap metabolic acidosis (can be hidden when pH is normal but mixed disorders are present). Compare △AG and △HCO3 to look for concurrent metabolic alkalosis or normal anion gap metabolic acidosis. Use a compensation chart/formula to reveal “overcompensation” or “undercompensation” which indicates the presence of another disorder.
- The presence of a normal pH with abnormal pCO2 and bicarbonate suggests a mixed acid-base disorder with counterbalancing acidosis and alkalosis.
- The pCO2 and serum bicarbonate typically move in parallel with an isolated acid-base disorder; both are high OR both are low. For example, a respiratory acidosis will have an increased pCO2 with a compensatory increase in serum bicarbonate. If the pCO2 and serum bicarbonate move in opposite directions (one high and one low), then you should consider the possibility of two simultaneous primary acid-base disorders (i.e., a mixed acid-base disorder).
- A mixed acid-based disorder consists of any combination of at least two disorders: two metabolic disturbances OR one respiratory and one metabolic. Triple acid-base disorders include one respiratory disorder (acidosis or alkalosis) with two metabolic disorders (high gap and normal gap metabolic acidosis OR high gap metabolic acidosis and metabolic alkalosis).
Assessment Of RTAs
Definition
- Renal tubular acidosis refers to an impaired acid-base metabolism by the kidney in the setting of normal glomerular filtration. These conditions are characterized by a non-elevated anion gap (hyperchloremic) metabolic acidosis.
- Kidney disease must be excluded as etiology of inappropriate acid-base metabolism.
- Chronic kidney disease (CKD) is associated with a non-elevated anion gap acidosis early in its course due to decreased generation of NH3 and decreased medullary trapping of NH4+.
- As CKD progresses, elevated anion gap acidosis tends to predominate as the kidney loses the ability to excrete anions (phosphate, sulfate, urate, etc.).
- Note: in the setting of acidemia, the expected urine pH is between 4.5-5.0 as virtually no HCO3 should be excreted.
Categories
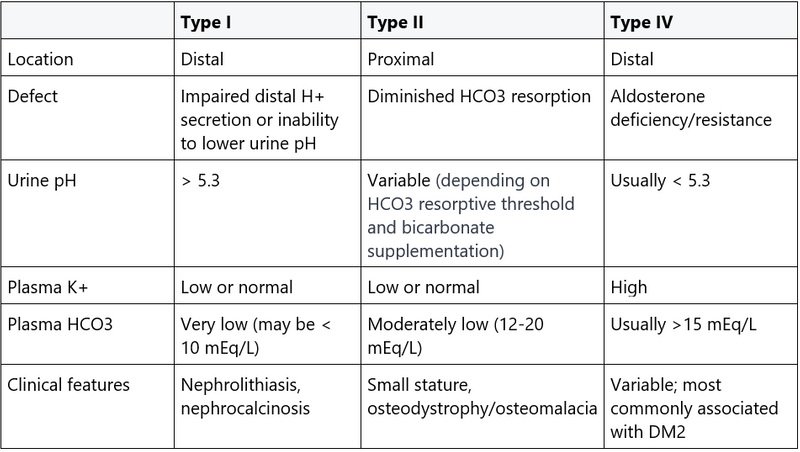
- Type I RTA (distal)
-
- Etiology: Type I RTA represents a failure to secrete H+ in the distal nephron, where urinary acidification takes place. This leads to metabolic acidosis with higher than appropriate urine pH, as the body is unable to acidify the urine to eliminate systemic acid.
- Causes
- Most common: in adult patients, urinary obstruction or Sjogren’s/SLE
- Primary (genetic)
- RA
- Myeloma
- Marked volume depletion
- Drugs
- Cyclosporine toxicity
- Amphotericin
- TMP/SMX can impair Na channels leading to a functional type I RTA. - Features/diagnosis
- Serum HCO3 may be <10 mEq/L as there is no way to excrete the acid load and bicarbonate is depleted by buffering the excess serum acid.
- Urine pH > 5.5, reflecting defect in urinary acidification. If a small amount H+ is secreted, it will be buffered by NH3.
-
- Type II RTA (proximal)
-
- Etiology: Type II RTA represents a failure to reabsorb filtered bicarbonate in the proximal tubule, causing substantial HCO3 wasting. Normally, reclamation of 80-90% of filtered HCO3 occurs in the proximal tubule; the distal nephron only absorbs a modest amount of bicarbonate.
- Causes
- Most common: for adult patients, multiple myeloma or nucleotide analogues (e.g., tenofovir), which causes a proximal tubule injury that manifests as Fanconi syndrome.
- Primary (genetic)
- Acetazolamide
- Heavy metals (Pb, Cd, Hg, Cu, others)
- Inherited and acquired Fanconi syndrome: generalized proximal tubular dysfunction with impaired ability to reabsorb one or more substrates that normally should be reabsorbed (e.g., bicarbonate, potassium, low molecular weight protein, glucose). It may be caused by any of the above etiologies. - Features/Diagnosis
- Serum HCO3 levels are usually maintained between 12-20 mEq/L. The serum HCO3 level approximates the tubule’s absorptive capacity: as the serum HCO3 level drops, the filtered load of HCO3 into the proximal tubule will decrease to the point that it can be fully reabsorbed.
- Urine pH can be variable, depending on the level of serum HCO3. Bicarbonate administration may affect the urine pH, as described below.
- If enough HCO3 is given, it may raise serum HCO3 level enough to overwhelm the reabsorptive capacity of the proximal tubule. This leads to HCO3 loss (spillover) in the urine, raising urine pH > 5.5.
- If serum HCO3 remains low, all of the filtered HCO3 can be reabsorbed, and there will be less HCO3 in the urine. Urine pH will be <5.3 due to normal H+ secretion by the functioning distal nephron.
- Look for accompanying electrolyte abnormalities in type II RTA, like hypokalemia, hypophosphatemia, and glucosuria.
-
- Type IV RTA- most common type of RTA in adults.
-
- Etiology: In Type IV RTA, aldosterone deficiency or resistance in the intercalated and principal cells of the distal nephron leads to hyperkalemia and impaired NH3/NH4+ production, thus causing metabolic acidosis.
- Causes
- Hypoaldosteronism-mediated
- Diabetic nephropathy (most common cause).
- Chronic interstitial nephropathy.
- Drugs (NSAIDS, heparin, ACEI/ARB, trimethoprim, calcineurin inhibitors).
- Addison's disease.
- Aldosterone-resistance mediated
- Sickle cell anemia (most common cause of aldosterone resistance).
- Urinary tract obstruction.
- Features/diagnosis
- Serum HCO3 usually > 15 mEq/L.
- Urine pH < 5.3. In contrast to type I RTA, there is insufficient NH3 production in type IV RTA, leaving the few H+ produced to be left unbuffered, thus leading to a lower urinary pH.
-
Evaluation
- Serum: ABG and CMP.
- Urine: UA/urine culture (UTI from urea-producing organisms can raise urine pH by metabolism of HCO3 and NH4+), urine lytes (Na, K, Cl).
- Can also use expanded urine lytes to calculate urinary osmolar gap (Na, Cl, K, BUN, glucose, osmolality); see discussion below.
- Serum potassium
- Hypokalemia: type II RTA (proximal) or type I RTA (distal).
- Hyperkalemic: type IV RTA (hypoaldosteronism) or type I RTA (distal). - Calculate urine anion gap (UAG):
- UAG is a surrogate for urine NH4+, the unmeasured cation in the urine.
- UAG = UNa + UK – UCl.
- UAG < 0 suggests extrarenal cause of normal anion gap metabolic acidosis. The kidney is appropriately compensating for the acidosis by secreting NH4+.
- UAG > 0 suggests renal cause (UAG may be negative in some cases of proximal RTA).
- UAG should not be used if there is excretion of another anion (lactate, DKA anions, etc.) OR if urine sodium <20 mEq/L (insufficient Na+ delivery to distal tubule does now allow for H+ exchange required for urinary acidification). - If urine sodium <20 mEq/L, consider calculating urine osmolal gap (UOG) instead.
- UOG = 2(UNa +UK) + Uurea/2.8 + Uglucose/18.
- UOG <50 is suggestive of RTA.
Treatment
- Type I and II: aggressive K supplementation followed by HCO3 supplementation (initial HCO3 supplementation can worsen hypokalemia, especially in proximal RTA).
- Use NaHCO3 or Na-citrate to replete.
- Bicarbonate goals
- Type I: normal serum HCO3.
- Type II: HCO3 >20 mEq/L. - Note: may also need close monitoring/repletion of calcium and phosphate.
- Type IV: treat hyperkalemia.
- Restrict dietary potassium, avoid potassium-sparing diuretics.
- Use loop diuretics and thiazides for potassium excretion.
- Can consider fludrocortisone in severe cases (recommend nephrology consultation before initiating).
Key Points
Cardiology
Rule out MI
Admit to Telemetry
-
Tele-nurse may reach out to you for > 6 PVCs/min, atrial fibrillation, ventricular fibrillation, > 3 beats of VT.
-
Admit as “observation status” if the patient will likely be discharged within 24 hours.
Activity
- Bed rest until ruled out (bedside commode okay for low-risk patient).
- Remember to promote ambulation once myocardial ischemia resolves.
Diet
- NPO except meds if possible cardiac catheterization or functional study in the AM. Applies to most patients, especially as ECGs and biomarkers are being trended.
- Hold beta-blockers before exercise or dobutamine stress testing.
- No nitrates or caffeine before vasodilatory (dipyridamole/ adenosine/regadenason) pharmacologic stress testing. Beta blockers are ok (but hold if unsure what type of test until am).
- Metformin should be held in all patients in case they need to undergo coronary angiography, place on SSI; theoretical risk for lactic acidosis
Nursing
- O2 via nasal cannula, starting at 2 L/min. Goal O2 > 95%.
- ECG on admission, trend as frequently as indicated (with symptoms, to capture evolving infarct, biomarker check, etc)
- CXR on admission.
- Chest pain protocol: vital signs, ECG, NTG 0.4 mg SL q5 minutes x 3, notify MD. ECG during and upon resolution of symptoms.
Labs
- Trend troponin ~q6-8hrs until peak, chem-panel, PT/PTT, lipids, TSH, and HgA1C
- CK-MB and myoglobin are not useful in diagnosis of ACS with contemporary troponin assays.
Medications
- Aspirin 325 mg PO (chewed), 81mg thereafter
- Statin: Atorvastatin 80 mg PO
- Β-blockers: Metoprolol tartrate 25-100 mg PO q12hr, consider IV if hypertensive. Target HR < 70. Avoid in bradycardia, severe bronchospasm or hypotension/concern for shock
- See Acute Coronary Syndrome: ST Segment Elevation or New LBBB for further details and contraindications.
- Pain Control (pain means ongoing ischemia/infarct):
- Reduce demand if indicated (blood pressure and heart rate control)
- Ensure proper anticoagulation (i.e. heparin is therapeutic); Plavix loading
- Nitrates (titrate up as needed): nitro SL (NTG 0.4 mg q5 minutes x 3)-> nitro paste -> nitro gtt (CCU level of care). Avoid in suspected RV infarct
- Morphine PRN (watchout for hemodynamic effects)
If in doubt, discuss with seniors!
Consult with cardiologist (i.e. catheterization, GP IIb/IIIa gtt, CCU care), especially for persistent chest pain in the concerning patient.
References
Amsterdam EA, Wenger NK, Brindis RG, et al. 2014 AHA/ACC Guideline for the Management of Patients With Non–ST-Elevation Acute Coronary Syndromes: A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines.J Am Coll Cardiol. 2014;64(24):e139-e228. doi:10.1016/j.jacc.2014.09.017.
Ibanez B et al. Effect of early metoprolol on infarct size in ST-segment-elevation myocardial infarcation patients undergoing primary percutaneous coronary intervention: the Effect of Metoprolol in Cardioprotection During an Acute Myocardial Infarction (METOCARD-CNIC) trial. Circulation. 2013;128(14):1495-503.
Meine TJ, Roe, MT, Chen AY, et al. Association of intravenous morphine use and outcomes in acute coronary syndromes: results from the CRUSADE Quality Improvement Initiative. Am Heart J 2005;149:1043-1049.
Chen ZM, Pan HC, Chen YP, et al, COMMIT (ClOpidogrel and Metoprolol in Myocardial Infarction Trial) collaborative group. Early intravenous then oral metoprolol in 45,852 patients with acute myocardial infarction: randomised placebo-controlled trial. Lancet 2005;366:1622-1632.
CHF
Definition
- A condition in which the heart is not able to pump enough blood to meet the body’s metabolic needs or does so in the face of elevated filling pressure due to abnormalities of ejection or abnormalities of filling.
Classification
- In patients presenting with new (or possibly unexplained worsening symptoms of heart failure), document systolic function with echocardiography (HFpEF vs HFrEF), and then exclude ischemic underlying etiology (MI or CAD) with angiography (Ischemic Dilated Cardiomyopathy vs Non-ischemic Dilated Cardiomyopathy).
- Classification of heart failure is important not only for more effective communication but for optimization of medical management
Overview of Heart Failure with Reduced Systolic Function
- Ischemic Etiologies: Coronary Artery Disease (major) and congenital coronary anomalies; myocardial bridging
- Non-Ischemic Etiologies: HTN, valvular heart disease, idiopathic, tachycardia mediated, toxins (EtOH, cocaine, meth, anthracyclines, etc), end-stage infiltrative disease (amyloid, hemochromatosis, sarcoid), endocrine (hypo/hyperthyroidism), myocarditis (viral, Chagas, HIV), radiation, peripartum, vitamin deficiencies (thiamine), genetic/familial,
- Etiologies of Exacerbations: poor dietary and/or medication adherence, myocardial ischemia, inadequate drug therapy, HTN, arrhythmia (e.g., atrial fibrillation), valvular heart disease, fluid overload, PE, infection, thyrotoxicosis, physical or emotional stress.
Evaluation of Acute Heart Failure
- Retrieve old ECHO, stress tests, ECGs, and cath reports.
- Take a thorough history (dyspnea, orthopnea, PND, edema, weight gain, abdominal discomfort, nausea, anorexia, baseline weight).
- Physical examination and clinical assessment:
- Is the patient warm or cold (reduced perfusion)? Look for fatigue, altered mental status, Cheyne-Stokes respiration, pallor, cool extremities, narrow pulse pressure, lactic acidosis, hyponatremia, renal failure.
- Is the patient dry or wet (congested)? (See chart below.)
- Left Sided Congestion (crackles, pulmonary edema, left ventricular S3, elevated JVP) +/- Right-sided congestion: elevated JVP, lower extremity edema, hepato-jugular reflex, pulsatile liver, right ventricular S3
- Labs: CBC, chem-10, coagulation studies, troponin, TSH, ECG (e/o ischemia, hypertrophy, pericarditis, new bundle branch block), CXR (vascular prominence, effusion, cardiomegaly).
- Diagnostic utility of B-type natriuretic peptide (BNP):
- BNP is released from the heart (mainly the LV) in response to increased wall tension.
- BNP measurement has limited utility after a good clinical assessment. If the diagnosis of HF is clinically apparent, a BNP test is not indicated. Measurement of BNP levels should not be used as a screening test. If the clinical picture is consistent with HF, do not let a low or normal BNP level necessarily deter appropriate diagnosis and therapy.
- In one study, BNP < 100 pg/mL was helpful in ruling out cardiac causes of dyspnea (<50 pg/mL had 96% negative predictive value for CHF) while BNP > 400 pg/mL is helpful for ruling in cardiac causes of dyspnea. For values <100 pg/mL and >400 pg/mL, consider other causes of dyspnea as well as CHF.
- The level of BNP correlates with the severity of HF. However, patients who are stable and well-compensated may run high BNP levels chronically.
- Obese patients have decreased BNP levels due to adipose clearance.
- Higher baseline levels of BNP are seen in older patients and women. BNP is falsely low in obesity, diuretics, ACEi, beta-blockers, and aldosterone antagonist use. BNP is low in constrictive pericarditis
Acute Management of Heart Failure Exacerbation.
Therapy should be tailored to the hemodynamic profile (Volume status vs Perfusion) as described below:
- Volume Overload (Wet) with Good Perfusion (Warm) -> Most common hospital presentation of CHF. IV diuretics ± nitrates, afterload reduction (ACEI/ARB, hydralazine, nitrates), ± aldosterone antagonists and beta-blockers when optimized.
- Volume Overload (Wet) with Poor Perfusion (Cold) -> Likely requires ICU care. IV diuretics, ± afterload reduction, ± inotropes/inodilators. In severe or refractory cases, sometimes PA catheter-guided therapy* is needed, PUF/CVVH, consideration of advanced therapies (LVAD, transplant evaluation).
- Non-volume Overload (Dry) with Poor Perfusion (Cold) -> Represents 10% of cases, challenging to treat. Often associated with cardio-renal syndrome. Inotropes/inodilators, afterload reduction, and advanced therapies can be considered.
- Non-volume Overload (Dry) with Good Perfusion (Warm) -> Compensated HF. Usually can be treated as an outpatient. Maintain volume status and prevent disease progression with rx. Chronic management with beta-blockers, ACEI/ARB, aldosterone antagonists, loop diuretics.
In general patients should be closely monitored:
- Telemetry monitoring (high risk for ventricular arrhythmia)
- Oxygen via NC or face-mask, goal >92% saturation. If needed, CPAP or BiPAP confers mortality benefit and reduces the need for mechanical ventilation.
- Monitor K, Mg, Cr (remember Cr may be elevated on admission secondary to venous congestion at the glomerulus; if HF-related, Cr should fall with diuresis). Do not hold diuretics for BP.
- Restrict sodium (<2g) and also fluids (<1500cc) if hyponatremic; daily weights, strict I&Os.
Overview and Specifics of Treatment
- Immediate Considerations: Diuresis, Inotropes, Afterload reduction
- Guideline Directed Therapy: ACE-i, Beta blockers, Aldosterone antagonists, Hydralazine/Nitrates
- Devices: ICD, CRT, CRT-D
- Advanced Therapies: Mechanical circulatory support, Transplant
Diuresis:
Loop diuretics:
- For Veno-dilation and natriuresis. With advanced right heart failure and diuretic resistance, use IV as oral absorption is diminished by bowel edema. Decongestion of hepatic and renal vascular beds will improve organ function. Reduction in LV wall stress and mitral regurgitation will improve cardiac output and BP.
- Initial dosing: 2.5 times normal oral diuretic dose (DOSE trial). If inadequate response (< 100 – 200mL UOP in first 30 mins), double dose and closely monitor UOP
- Consider furosemide/bumex gtt in patients with severe volume overload and/or sub-optimal response to bolus dosing of diuretics.
- Furosemide gtt: Give initial 20-80 mg IV bolus (higher doses for patients with worse renal function; lower doses for diuretic naïve patients). Then start gtt at 5 mg/hr (range 5-20 mg/hr). FENa can be monitored to determine effectiveness of natriuresis (maximum FENa = 20%).
- Bumex gtt: Give initial 1-2 mg bolus. Then start bumex gtt at 0.5 mg/hr (range 0.2-2 mg/hr).
- If inadequate diuresis with loop diuretic alone, try adding a thiazide diuretic such as chlorothiazide IV/PO 125-500 mg or metolazone 2.5-10 mg PO, diuril IV dosed 30 min before the loop diuretic. Metolazone PO should precede IV loop diuretic by at least 2-4 hours. Monitor serum electrolytes (Na, K+, and Mg2+) closely, replete as necessary.
- Markers of adequate diuresis include resolution of dyspnea, decreased JVP, Cr normalization, return to baseline weight. JVP should be closely monitored to avoid ‘bumping patient’s creatinine.’
- Transition to PO diuretics and monitor response to PO prior to discharge
Ultrafiltration:
Fluid removal with no effect on serum electrolytes, consideration reserved for in cases of acute decompensated heart failure inadequately responsive to aggressive diuretic regimen. Increased risk of serious adverse advents and no difference in weight loss at 96 hours when compared to pharmacologic therapy (CARRESS-HF).
Optimizing Hemodynamics/Inotropes:
Dobutamine:
- Beta-adrenergic agonist (predominantly beta-1), inotrope, mild arterial vasodilator. Generally the inotrope of choice in cardiogenic shock.
- Minimal effects on left sided filling pressures. At higher doses (>10-15 mcg/kg/min) can exert significant alpha-adrenergic activity increasing SVR and worsening forward flow. Effectiveness curtailed with concomitant beta blockers.
- Adverse effects: increased myocardial oxygen demand, hypotension, ventricular arrhythmias
- Tolerance can develop with beta receptor down-regulation.
- Normal dose range: 2.0-5.0 mcg/kg/min, can be run peripherally
- Titrate to UOP, CO, SvO2 if a right heart catheter is in place.
Dopamine:
- Low dose acts through dopamine receptors increasing renal blood flow and natriuresis (1-3 µg/kg/min). Intermediate doses act through beta-adrenergic receptors to increase HR and contractility (2-10 µg/kg/min). High doses stimulate alpha-adrenergic receptors increasing afterload, this may be detrimental in HF (>10 µg/kg/min).
- Use only to stabilize hypotensive patients.
- Can run peripherally for <24 hours as long as a viable PIV has been established
Milrinone:
- Phosphodiesterase-3 inhibitor, inodilator
- Hemodynamic profile: Reduces right- and left-sided filling pressures, reduces pulmonary and systemic vascular resistance, direct positive inotropic effect. Longer half-life than dobutamine, more effective in beta-blocked patients and suspected dobutamine unresponsiveness due to beta receptor down-regulation.
- Adverse effects: Toxicity profile similar to dobutamine, although slightly less tachycardia and myocardial oxygen demand.
- Normal dose range: 0.375-0.75 mcg/kg/min; starting dose in renal dysfunction is 0.25 mcg/kg/min.
- Do not give a bolus prior to starting infusion even though doing so is suggested in the package insert. Bolus dosing is associated with more hypotension and is rarely indicated.
Digoxin:
- Na-K-ATPase inhibition improves contractility, anti-andrenergic effect also beneficial. The only safe PO inotrope. Symptomatic improvement and decrease in hospitalizations, but no mortality benefit in HF (DIG trial).
- Normal dose range: 0.125-0.25 mg daily, loading dose not indicated in HF.
- Optimal serum concentrations: 0.5-0.8 ng/mL in men, 0.5-0.9 ng/mL in women
- Adverse effects: confusion, visual disturbances, arrhythmias (conduction disease, pAT)
Nitrates:
- Preferential venodilator useful in acute setting to reduce pulmonary edema and other congestive symptoms. Reduces LV filling pressure and SVR.
- Sublingual, nitropaste, or IV nitroglycerin (start at 10-20 mcg/min and titrate as permitted by BP).
- When stable, convert to PO nitrate (e.g. start with isosorbide dinitrate 10 mg PO TID).
- Avoid with concurrent PDE-5 inhibitor, NO reductase inhibitor, severe aortic stenosis, cyanide toxicity.
- Adverse effects: headache (common), hypotension, tachyphylaxis
Guideline-Directed Therapy
ACE inhibitors:
- For afterload reduction and neuro-hormonal effects. Have a proven mortality benefit (CONSENSUS trial), prevent re-hospitalization, stop adverse LV remodeling in chronic HF (SOLVD trial). This effect is independent of the anti-hypertensive effect.
- If ACE inhibitor causes cough, try ARB (angiotensin II receptor blocker). Always attempt re-challenge with ACE inhibitor in future as ACE confers improved mortality benefit over ARB.
- Dosing: Captopril 3.125 – 6.25 mg PO q8hr and increase dose by dose as BP permits.
- Monitor K+, and Cr (up to 30% increase in Cr is acceptable).
- Once stable, switch to equivalent dose of once-daily ACE inhibitor.
- Target dosing: Lisinopril 40mg PO Qday.
Beta-blockers:
- For hemodynamic benefits, beneficial LV remodeling, decreasing frequency of PVCs. Multiple trials showing mortality benefit, reduced hospitalizations, symptom mitigation (MERIT-HF, PRECISE, CIBIS-I & II, etc.).
- Metoprolol ER, carvedilol, and bisoprolol have symptom and mortality benefit and slow disease progression for NHYA class II-IV chronic HF.
- Do not initiate in acute setting (OPTIMIZE-HF trial). Once patient is adequately diuresed, initiate beta blocker with appropriate up-titration on outpatient basis.
- Do not withdraw in exacerbation unless patient is hypotensive or in cardiogenic shock.
- Initial dosing: Start with metoprolol ER 12.5-25 mg PO daily or carvedilol 3.125 mg PO BID and titrate up as permitted by HR and BP.
- Target dosing: Metoprolol ER 200 mg daily or carvedilol 25 mg BID (50 mg BID if > 85 kg). COMET trial showed greater benefit with carvedilol vs. short-acting metoprolol. Also recent work showed that HR may be more important than final dose.
Aldosterone Antagonists:
- Survival benefit derived from potassium sparing action lowering risk of hypokalemia-associated arrhythmia as well as blocking of mineralocorticoid activity.
- Indicated for the following populations:
- NYHA class II HF + LVEF ≤ 30% (EMPHASIS-HF trial)
- NYHA class III-IV HF + LVEF < 35% (RALES trial)
- recent MI + LVEF ≤ 40% + symptomatic HF or DM (EPHESUS trial)
- Contraindications: Cr > 2.5 mg/dL in men, Cr > 2.0 mg/dL in women, K+ > 5 meq/L.
- Initial dosing: Spironolactone 25 mg daily (every other day dosing for eGFR < 50 mL/min), titrate up to 50 mg daily if K+ < 5 meq L at 4 weeks.
- Target dosing: Spironolactone 25-50 mg daily
- Can consider changing to eplerenone (much more expensive) if undesired endocrine side effects (e.g. gynecomastia) with spironolactone.
- Monitor K+.
Hydralazine + Nitrates:
- Hydralazine is a preferential arterial vasodilator.
- Indicated for black patients with NYHA class III-IV HF and LVEF < 40% on maximal medical therapy.
- Initial dosing: Hydralazine 25 mg TID + isosorbide dinitrate 20 mg TID or combination isosorbide dinitrate-hydralazine 37.5 mg-20 mg TID. Titrate up every 2-4 weeks as permitted by BP.
- Target dosing: Hydralazine 75 mg TID + isosorbide dinitrate 40 mg TID.
- Can consider isosorbide mononitrate (30-120 mg daily) as alternative to TID-dosed isosorbide dinitrate.
ICD and CRT
Indicated only after medical optimization and removal of applicable vices (no active drug use) – please see applicable section.
Implantable cardiac defibrillator (ICD): Primary prevention of sudden cardiac death in populations at increased risk for life-threatening ventricular arrhythmias. Mortality benefit for NYHA class II-III HF + LVEF ≤ 35% despite optimal medical management for at least 3 months (SCD-HeFT trial).
Cardiac resynchronization therapy (CRT): HF frequently leads to intraventricular conduction delay and ventricular dyssynchrony. Resynchronization (biventricular pacing) improves pump function with mortality benefit, symptom improvement, and decreased hospitalizations for NYHA class II-III HF + LVEF ≤ 35% + LBBB + QRS ≥ 150 ms despite optimal medical management (MIRACLE, CARE-HF, COMPANION, MADIT-CRT trials).
Most patients who meet criteria for ICD also meet criteria for CRT and vice versa. Combination devices (CRT-D) confer superior mortality benefit when compared to ICD or CRT alone (REVERSE, MADIT-CRT, COMPANION trials).
Advanced Therapies
Mechanical circulatory support
- Intra-aortic balloon pump (IABP): Temporary treatment for HF refractory to medical management, systolic unloading and improved coronary perfusion, particularly useful in patients with ischemia or mitral regurgitation, placed in cath lab (see corresponding section).
- Left ventricular assist device (LVAD): Can be used as a bridge to recovery, a bridge to transplant, or “destination” therapy for outpatient use. Placed in OR.
Cardiac transplantation: Consider early involvement of transplant/advanced HF team in patients with new, rapidly progressive, severe HF, or advanced HF refractory to treatment.
Overview and Management of Heart Failure with Preserved Systolic Function
Etiologies
- Etiologies include: ischemic heart disease (most common), hypertensive heart disease, diabetic cardiomyopathy, high output cardiac failure (e.g., severe anemia, AV fistulae, thyrotoxicosis), restrictive cardiomyopathy (radiation injury, infiltrative disease [e.g., amyloidosis], metabolic storage disease [e.g., Fabry’s disease], endocardial fibrosis), and hypertrophic cardiomyopathy, valvular heart disease (e.g., AS, MR). Exclude HF due to constrictive pericarditis or due to isolated right heart failure (pulmonary HTN, cor pulmonale)
- Etiologies of exacerbation: Anything that increases LV wall stiffness will predispose to exacerbation of diastolic HF. Common precipitants include ischemia, tachyarrythmia, HTN.
Evaluations
- CBC (anemia), chem-10 (CKD), LFTs (cirrhosis), TFTs (thyrotoxicosis), lipid panel, A1c, urine microalbumin, SPEP/UPEP as indicated
- Diastolic dysfunction can be assessed non-invasively by echo (LVH, impaired filling, valve disease, atrial enlargement, rule out constrictive pericarditis) or invasively by cardiac catheterization.
- If echo is unrevealing, consider cardiac catheterization to evaluate for occult arterial disease and, occasionally, endomyocardial biopsy.
- On exam, look for HTN, S4, signs of LVH.
Treatment
- Similar to treatment for systolic HF as outlined above. Address underlying etiology (ischemia, HTN, infiltrative process, etc)
- Evidence is weak for guiding treatment with commonly used drugs for systolic failure; many studies show marginal or no benefit, nevertheless optimization is important.
- Treat congestion (diuretics, ultrafiltration/dialysis, salt restriction)
Discharge Planning
- All HF patients should receive the pneumococcal and influenza vaccines.
- Advance directive education, palliative care involvement (depending on severity and co-morbities), goals of care discussions for patients with recurrent hospitalizations.
- Early outpatient follow-up and/or telephone nurse follow-up after discharge help reduce readmissions.
- Heart failure education, including dietary modification (fluid and salt restriction), scale and instruction regarding daily weights, diuretic self-titration teaching, avoidance of cardio-toxic recreational drugs, explain rational of all medications.
References
Felker GM et al. Diuretic strategies in patients with acute decompensated heart failure. N Engl J Med 2011;364(9):797-805.
Jessup M, Brozena S. Heart failure. N Engl J Med 2003 348:2007-2018.
Kadish A, Mehra M. Heart Failure Devices: Implantable Cardioverter-Defribillators and Biventricular Pacing Therapy. Circulation 2005;111:3327-3335.
McMurray JJ, Pfeffer MA. Heart failure. Lancet 2005;365:1877-1889.
Najjar S. Heart Failure with Preserved Ejection Fraction. J Am Coll Cardiol 2009;54: 419-421.
Owan TE et al. Trends in prevalence and outcome of heart failure with preserved ejection fraction. N Engl J Med 2006 Jul 20; 355:251-9.
Rathore SS, Curtis JP, Wang Y, et al. Association of serum digoxin concentration and outcomes in patients with heart failure. JAMA 2003;289:871-878.
Endocarditis
Overview
Diagnosis requires 2 major, 1 major with 3 minor, or 5 minor criteria from the modified Duke Criteria listed below:
MAJOR CLINICAL CRITERIA:
- Persistently positive blood cultures with typical IE organisms. Bacteremia is continuous and high grade. Two blood cultures are positive > 90% of the time. Repeat the blood cultures every 48 hours until sterile. Prevalence of endocarditis among patients with S. aureus bacteremia is approximately (13-25%); TTE is now recommended in all patients with S. aureus bacteremia.
- Evidence of valvular vegetation, or abscess, or dehiscence on TEE/TTE.
- New regurgitant murmur.
- Serologic dx (Coxiella IgG titer >1:800 or positive Bartonella or C.psittaci titers) or single positive culture of Coxiella burnetii (Q fever).
MINOR CLINICAL CRITERIA:
- Predisposing condition (see below).
- Fever (temperature >38.0 C).
- Vascular events (septic emboli, pulmonary emboli, mycotic aneurysm, CNS or conjunctival, and Janeway lesions).
- Immunologic events (Osler’s nodes, glomerulonephritis, Roth spots, + Rheum Factor).
- Microbiologic data not meeting major criteria.
Etiology / Risk Factors
Predisposing conditions include prosthetic valves, previous IE, IDU, structural heart disease (e.g., valvular abnormalities including MV prolapse), hemodialysis and indwelling catheters.
Evaluation
- Clinical manifestations are inconsistent, so suspect the condition in those with risk factors. Fever may be absent in up to 10% of patients. 70% have heart murmurs (50% new murmur, 20% worsening of old murmur). Only ~10% of patients have classic peripheral stigmata of endocarditis (Janeway lesions, Osler nodes, splinter hemorrhages).
- Physical Exam
- Cardiac: exam can be dynamic so reassess for new or changing regurgitant murmurs.
- Skin: the most common rash is petechiae; can be on the conjunctiva, palate, or buccal mucosal surfaces. Splinter hemorrhages are non-blanching, often at distal nail bed. Osler nodes are small tender nodules on fingers and/or toes. Janeway lesions are small, macular, painless hemorrhages on palms or soles.
- Eyes: Roth spots are pale, oval retinal lesions surrounded by hemorrhage.
- Full neurologic exam to document baseline and to evaluate for focal findings.
- Other: evaluate for arthritis, vertebral tenderness, and tender splenomegaly.
- Microbiology for native versus prosthetic valves differs slightly, although Staph aureus is the most common organism in both.
- Early vs Late prosthetic valve infections: early infections are typically acquired from surgical-related bacteremia within days to weeks. Because the valve and sutures are not yet endothelialized, bacteria easily adhere to these surfaces. They are more likely to cause valve dehiscence or abscess.
- Early organisms (<2 mo): Staph > CoNS (Staph epidermidis).
- Late organisms: CoNS and Staph aureus are roughly equivalent.
- Infections in valves > 12 mo after surgery are similar to those of native valves, with the exception of bioprosthetic valves, which may breakdown over time and become more susceptible to infection.
- Echo: in native valve endocarditis, the sensitivity of TTE is ~60% and TEE is ~90%. Specificity is ~99% for both. Guidelines recommend TEE first but practically, we usually begin with TTE and consider TEE if negative if there remains a high pre-test probability. Consider TEE in patients with:
- High concern for native-valve endocarditis and a negative TTE.
- Prosthetic valves (TTE is 15-30% sensitive), cardiac device (e.g. pacemaker, AICD) or prior IE.
- Limited thoracic windows (obesity, COPD, mechanical ventilation).
- Concern for perivalvular complications (e.g. myocardial abscess).
- Culture negative endocarditis: defined as negative cultures after 7 days. One of the most common causes is antibiotic administration before cultures. The most common infectious causes in America are Bartonella spp and Coxiella burnetii (Q fever). Other pathogens: Chlamydia, Legionella, Brucella. Note, the HACEK organisms are no longer a common cause of culture negative endocarditis as they can be cultured by most microbiology labs.
Management
- All patients need prolonged courses of antibiotics and may need surgery.
- ID should be consulted for all cases of documented endocarditis.
- Empiric therapy for native valve IE in most patients is vancomycin (targeted to a goal trough of 15-20) plus ceftriaxone 2gm IV q24h, started after cultures have been drawn. Subsequently tailor antibiotics to culture results.
- Oral antibiotic step-down therapy: Not yet standard of care but POET (https://www.nejm.org/doi/full/10.1056/NEJMoa1808312) study found that oral step down therapy was noninferior in their population to full-course IV therapy. Caveats included only Streptococcus, MSSA, CoNS, or Enterococcus faecalis organisms and few PWID.
- Surgical indications in native valves include:
- Valve dysfunction (i.e. aortic or mitral) causing heart failure.
- Perivalvular extension with development of abscess, fistula, and/or heart block.
- Fungi or orther highly resistant organisms that are difficult to treat with antibiotics alone.
- Persistent bacteremia despite maximal treatment, indicating a lack of source control.
- Recurrent embolization with persistent vegetations despite appropriate treatment.
- Large vegetations (>1cm) with severe valvular regurgitation (Kang et al, NEJM 2012).
- Complications: suspect with persistent fever for > 48 hours despite treatment or persistent bacteremia despite appropriate treatment.
- Cardiac: remember to obtain baseline ECG to assess for heart block or conduction delay (e.g. PR prolongation) due to perivalvular abscess (more common in aortic valve disease). Other complications include cardiac ischemia (embolism to coronary ostia). Heart failure is now the most common cause of death in endocarditis.
- Embolic: systemic embolization is usually due to left-sided endocarditis or via PFO. Can occur in up to 30% of patients with Staph aureus endocarditis. Risk factors include S. aureus, S. bovis, mitral valve disease, veg > 10mm and increased veg mobility on echo. While a history of aspirin use may be protective, starting anti-platelet treatment after diagnosis may cause increased bleeding (e.g. hemorrhagic conversion of septic emboli) and is not recommended.
- Persistent fever: while on antibiotics for endocarditis: consider metastatic infection including abscess (splenic, perivalvular, renal, and psoas), septic pulmonary emboli, pleural effusion, CNS infection, vertebral osteomyelitis, septic arthritis (esp. sacroiliac, pubic, manubriosternal joints), drug fever, and catheter-associated phlebitis.
Key Points
- Predisposing factors include prosthetic valves, previous IE, IDU and catheters.
- Monitor for EKG changes, evidence of heart failure and systemic emboli.
- The microbiology for native versus prosthetic valves differs slightly, although Staph aureus is the most common organism in both.
- Consider surgery in cases of heart failure, severe AI/MR, fungi or highly resistant organisms, perivalvular disease, >10mm mobile vegetation, or failed medical therapy.
References
Baddour LM, Wilson WR, Bayer AS, et al. Infective endocarditis in adults: diagnosis, antimicrobial therapy, and management of complications: a scientific statement for healthcare professionals from the American Heart Association. Circulation 2015 Oct 13;132(15):1435-86.
Durack DT, Lukes AS, Bright DK. New criteria for diagnosis of infective endocarditis: utilization of specific echocardiographic findings. Duke Endocarditis Service. Am J Med 1994;96:200-209.
Fowler VG Jr, Miro JM, Hoen B, et al. Staphylococcus aureus endocarditis: a consequence of medical progress. JAMA 2005;293:3012-3021.
Li JS, Sexton DJ, Mick N, et al. Proposed modifications to the Duke criteria for the diagnosis of infective endocartiditis. Clin Infect Dis 2000;30:633-638.
Murdoch DR et al. Clinical presentation, etiology, and outcome of infective endocarditis in the 21st century: the International Collaboration on Endocarditis-Prospective Cohort Study. Arch Intern Med. 2009;169:463-73.
Hoen B, Duval X. Clinical practice. Infective endocarditis. N Engl J Med 2013; 368:1425–33.
Wang A et al. Contemporary clinical profile and outcome of prosthetic valve endocarditis. JAMA. 2007;297:1354-61.
Kang et al, Early Surgery versus Conventional Treatment for Infective Endocarditis, N Engl J Med 2012; 366;26: 2466-73.
Iversen K, Ihlemann N, Gill SU, et al. Partial Oral versus Intravenous Antibiotic Treatment of Endocarditis. N Engl J Med. 2019 Jan 31;380(5):415-424.
EKG reading made easy
Rates
- Normal: 60-100 bpm
- Tachycardia: > 100 bpm
- Bradycardia: < 60 bpm
Readings
- Count the number of large squares present within one R-R interval.
- Divide 300 by this number to calculate heart rate.
OR
- Count the number of complexes on the rhythm strip (each rhythm strip is typically 10 seconds long).
- Multiply the number of complexes by 6 (giving you the average number of complexes in 1 minute).
Note:
- A patient’s heart rhythm can be regular or irregular.
- Irregular rhythms can be either:
- Regularly irregular (i.e. a recurrent pattern of irregularity)
- Irregularly irregular (i.e. completely disorganized)
The cardiac axis
The cardiac axis describes the overall direction of electrical spread within the heart.
In a healthy individual, the axis should spread from 11 o’clock to 5 o’clock.
To determine the cardiac axis you need to look at leads I, II, and III.
Right Axis deviation
- Right axis deviation (RAD) involves the direction of depolarisation distorted to the right (between +90º and +180º).
- The most common cause of RAD is right ventricular hypertrophy. Extra right ventricular tissue results in a more robust electrical signal being generated by the right side of the heart. This causes the deflection in lead I to become negative and the deflection in lead aVF/III to be more positive.
- RAD is commonly associated with conditions such as pulmonary hypertension, as they cause right ventricular hypertrophy. RAD can, however, be a normal finding in very tall individuals.
Left Axis deviation
- Left axis deviation (LAD) involves the direction of depolarisation distorted to the left (between -30° and -90°).
- This results in the deflection of lead III becoming negative (this is only considered significant if the deflection of lead II also becomes negative).
- Conduction abnormalities usually cause LAD.
P Wave
The next step is to look at the P waves
- Sawtooth baseline → flutter waves
- Chaotic baseline → fibrillation waves
- Flatline → no atrial activity at all
- The PR interval should be between 120-200 ms (3-5 small squares).
Note: A prolonged PR interval suggests the presence of atrioventricular delay (AV block).
If the PR interval is shortened, this can mean one of two things:
- the SA node is not in a fixed place and some people’s atria are smaller than others.
- an accessory pathway and can be associated with a delta wave (see below which demonstrates an ECG of a patient with Wolff Parkinson White syndrome).
QRS Complex
When assessing a QRS complex, you need to pay attention to the following characteristics:
- Width
- Height
- Morphology
Width can be described as NARROW (< 0.12 seconds) or BROAD (> 0.12 seconds)
Height can be described as either SMALL or TALL:
- Smallcomplexesare is defined as < 5mm in the limb leads or < 10 mm in the chest leads.
- Tallcomplexesimply ventricular hypertrophy (although can be due to body habitus e.g. tall slim people).
To assess morphology, you need to assess the individual waves of the QRS complex.
Note – the presence of a delta wave does NOT diagnose Wolff-Parkinson-White syndrome. This requires evidence of tachyarrhythmias AND a delta wave.
Q Wave
Isolated Q waves can be normal.
A pathological Q wave is > 25% the size of the R wave that follows it or > 2mm in height and > 40ms in width.
R Wave
Assess the R wave progression across the chest leads (from small in V1 to large in V6).
The transition from the S > R wave to the R > S wave should occur in V3 or V4.
Poor progression (i.e. S > R through to leads V5 and V6) can be a sign of previous MI but can also occur in very large people due to poor lead position.
ST-Segment
The ST segment is the part of the ECG between the end of the S wave and the start of the T wave.
In a healthy individual, it should be an isoelectric line (neither elevated nor depressed).
ST-elevation is significant when it is greater than 1 mm (1 small square) in 2 or more contiguous limb leads or >2mm in 2 or more chest leads. It is most commonly caused by acute full-thickness myocardial infarction.
ST depression ≥ 0.5 mm in ≥ 2 contiguous leads indicates myocardial ischemia.
T Waves
T waves are considered tall if they are:
- > 5mm in the limb leadsAND
- > 10mmin the chest leads (the same criteria as ‘small’ QRS complexes)
Tall T waves can be associated with:
- Hyperkalaemia(“tall tented T waves”)
- HyperacuteSTEMI
Inverted T waves in other leads are a nonspecific sign of a wide variety of conditions:
- Ischaemia
- Bundle branch blocks (V4-6 in LBBB and V1-V3 in RBBB)
- Pulmonary embolism
- Left ventricular hypertrophy (in the lateral leads)
- Hypertrophic cardiomyopathy (widespread)
- General illness
Flattened T waves are a non-specific sign, that may represent ischemia or electrolyte imbalance.
Biphasic T waves have two peaks and can be indicative of ischemia and hypokalaemia.
U Waves
U waves are not a common finding.
The U wave is a > 0.5mm deflection after the T wave best seen in V2 or V3.
These become larger the slower the bradycardia – classically U waves are seen in various electrolyte imbalances, hypothermia and secondary to antiarrhythmic therapy (such as digoxin, procainamide, or amiodarone).
References
- James Heilman, MD. Fast atrial fibrillation. Licence:CC BY-SA 3.0.
- Michael Rosengarten BEng, MD.McGill. Right axis deviation. Licence:CC BY-SA 3.0.
- James Heilman, MD. Mobitz type 2 AV block. Licence:CC BY-SA 3.0.
- James Heilman, MD. Complete heart block. Licence:CC BY-SA 3.0.
- James Heilman, MD. Delta wave. Licence:CC BY-SA 3.0.
- Michael Rosengarten BEng, MD.McGill. Q-waves. Licence: CC BY-SA 3.0.
- Michael Rosengarten BEng, MD.McGill. Poor R-wave progression. Licence:CC BY-SA 3.0.
- Michael Rosengarten BEng, MD.McGill. Tall tented T-waves. Licence: CC BY-SA 3.0.
- T-wave morphology. Licence:CC BY-SA 3.0.
- James Heilman, MD. U-wave. Licence:CC BY-SA 3.0.
- Michael Rosengarten BEng, MD.McGill. Left axis deviation. Licence:CC BY-SA 3.0.
Syncope
Syncope
- Rapid onset of transient loss of consciousness
- Inability to maintain postural tone
- It may be associated with a fall
- Resolves spontaneously and quickly without intervention
Presyncope (Near-Syncope)
- Weakness, Dizziness, lightheadedness, or "graying out" of consciousness without loss of postural tone
- Evaluate Presyncope with the same vigor as Syncope
- Presyncope has the same risks of adverse events as Syncope
Causes: Neural or Reflex Mediated Syncope (no cardiovascular risk, most common, 45% of cases)
- Vasovagal Syncope (Vasodepressor Syncope)
- Situational Syncope
- Carotid Sinus Syncope
- Glossopharyngeal neuralgia (uncommon)
- Trigeminal Neuralgia
- Hypovolemia
- Medication-related Syncope (Drug-Induced Syncope, responsible for 5-15% of Syncope causes)
- Recreational drug use
- Postural Tachycardia Syndrome (POTS)
- Most common in young female women (associated with chronic Fatigue and Mitral Valve Prolapse)
10. Autonomic failure
Cardiac syncope
- Arrhythmias
- Ventricular Tachycardia
- Sick Sinus Syndrome
- Supraventricular Tachycardia
- Atrioventricular Block (second or third degree)
- Pacemaker malfunction
- Valvular disorders
- Hypertrophic Cardiomyopathy (esp. young patients)
- Aortic Stenosis
- Acute Mitral Valve Regurgitation (i.e. acute MI with papillary Muscle rupture)
- Prosthetic Heart Valve complications (e.g. Thromboembolism, valvular obstruction)
Vascular disorders
- Myocardial Infarction
- Aortic Dissection
- Abdominal Aortic Aneurysm rupture
- Pulmonary Embolism
- Pulmonary Hypertension
- Subarachnoid Hemorrhage
- Subclavian Steal Syndrome
Myocardial disorders
- Hypertrophic Cardiomyopathy
- Atrial myxoma
Examination
- Vital sign
- General
- Cardiovascular examination-murmurs, Carotid bruit, asymmetric pulses
- Abdomen and pelvis exam- pulsatile mass and decreased femoral pulses, pelvic pain, rectal exam
Labs
- Basic Chemistry Panel (Serum Electrolytes including Glucose)
- Hemoglobin or Hematocrit
- Pregnancy Test (urine HCG)
- Fecal Occult Blood Test
- Troponin I
- D Dimer if necessary.
Diagnostics
- Electrocardiogram (EKG)
- Continuous cardiac monitoring-telemetry for inpatient
Imaging
- Chest XRay
- Echocardiogram
- CT chest with contrast (if Pulmonary Embolism is suspected)
- Imaging related to injuries sustained in a Syncope- fall
- CT Head (usually low yield except indicated by history and physical examination)
Indications for head imaging include:
- Age over 65 years
- Warfarin use
- First Seizure
- Trauma above the clavicles
- Persistent neurological deficit
- Dizziness
- Sudden onset headache (Thunderclap Headaches)
Note: The San Francisco Syncope Rule (CHESS Score) or Canadian syncope risk score are used to evaluate the short-term risk of severe outcomes and may reduce the syncope hospitalization rate.
Management depends on the cause
- Fall precautions
- Telemetry if needed
- Assess ability to tolerate PO
- IV fluids if needed
- Consider intoxication
References
- Joshi and Dermark (2016) Crit Dec Emerg Med 30(8):3-12
- Orman and Mattu in Herbert (2016) EM:Rap 16(3): 9-11
- Orman and Mattu in Herbert (2018) EM:Rap 18(6): 10-11
- Schauer et al. (2016) Crit Dec Emerg Med 30(9):13-9
- Kapoor (2000) N Engl J Med 343:1856-62 [PubMed]
- Brignole (2001) Eur Heart J 22:1256-306 [PubMed]
- Miller (2005) Am Fam Physician 72:1492-500 [PubMed]
- Runser (2017) Am Fam Physician 95(3): 303-12 [PubMed]
- Vermeulen (2007) Stroke 38(4): 1216-21 +PMID: 17322078 [PubMed]
Endocrinology
DKA
Diagnosis
DKA vs HHS:
- DKA sugar ranges from 250 to 500 mg/dL
- HHS typically has sugars > 600 mg/dL
- Serum osmolality > 320 in HHS
- Neurologic symptoms such as stupor and coma are primarily seen in HHS, but can sometimes be seen in severe DKA.
- Little to no ketonuria/ketonemia in HHS
- Anion gap mainly in HHS
There may be focal neurological deficits and/or seizures in HHS.
In DKA, there may be nausea, vomiting, and abdominal pain. The delayed gastric emptying and/or ileus caused by acidosis and electrolyte derangement may be a cause for such symptoms.
Kussmaul respirations are indicative of acidosis since this is a compensatory mechanism. A fruity breath may be from acetone, which is one of the three ketone bodies produced.
Infection or inadequate control of DM are the main causes. Sometimes DKA is the first presentation for DM.
Laboratory and Ancillary Testing
First assess clinical stability of the patient. Ability to protect airway and mental status assessment are important assessments.
A part of the quick assessment is the following STAT orders… (these should already be ordered by ED, but always make sure these are ordered when you accept an admission)
- Basic metabolic panel
- Urine analysis
- Venous blood gases
- Beta Hydroxybuterate level
- CBC
- CXR (if respiratory symptoms)
- Influenza panel (if in season)
- Blood cultures (if septic)
* remember that in DKA the total water deficits are 6L and for HHS 9L.
Common Laboratory Derrangements
Hyponatremia is often present due to fluid shifting from ICF to ECF. Basically the hyperglycemia causes fluid shifts from ICF to ECF. Be cautious of patients with impaired thirst mechanisms and the summer months where hot weather can cause dehydration.
For every 100 mg/dL increase in serum glucose, expect a 2mEq/L fall in serum sodium.
Hypokalemia or hyperkalemia can be present. Increased osmotic diuresis due to hyperglycemia can cause losses of potassium. Conversely, elevated potassium can be cause by ICF to ECF shifts of potassium due to lack of insulin or significant insulin resistance.
Hypophosphatemia or hyperphosphatemia is present. Dietary causes such as low phosphate intake can be present in uncontrolled DM. Conversely, hyperphosphatemia can be present in metabolic acidosis and hyperglycemia due to ICF to ECF shifts of phosphate.
Lipase and amylase are often elevated and DKA can masquerade as pancreatitis. Clinical judgement is necessary to distinguish the two.
Leukocytosis is present in many DKA or HHS patients. Hypercortisolemia and metabolic potentiators such as excess catecholamines can cause this. Think stress response. Do not forget to think about infectious etiology, WBC > 25K or bandemia with > 10%.
Acute Kidney Injury in the form of increased creatinine or reduced GFR can be present. In this case think dehydration or hypovolemia.
Hyperlipidemia can be present and increased lipolysis can serve as substrates for ketone body generation.
DKA and HHS are treated the same for the most part. It is important to think of the four hallmarks of DKA and HHS treatment which are correction of …
- Hyperglycemia
- Electrolyte derangement
- Acidosis
- Dehydration
Use the order set in the hospital
- Fluid Replacement
a. In the first 2 hours, isotonic (Normal Saline) fluid boluses (1L/hr in average sized person). Be cautious and individualize care on CHF or fluid intolerant patients.
b. In the 3rd hour, continue fluids using either normal saline or half normal saline. If sodium is below reference range, use NS at 250 to 500 mL/hr. If sodium is normal or above reference range, then half normal.
2. Insulin gtt (regular insulin)
a. 0.1 units/kg bolus followed by 0.1 units/kg/hr.
b. If no bolus is used, then 0.14 units/kg/hr.
c. Nursing will adjust rate based on serial glucose measurements.
Caution – if potassium is < 3.3, correct the hypokalemia first otherwise you will tank the patient’s potassium which is dangerous.
Management and Monitoring
3. Electrolytes – there is a protocol for electrolyte correction on the hospital order set. Be sure to use this.
a. Potassium – again replete potassium first if value is < 3.3. May need to add KCl to replacement fluids above (20 to 40 mEq/hr) if potassium is between 3.3 and 5.5 mEq/L.
b. Sodium – this will correct with correction of hyperglycemia.
c. Phosphorus – Correct when <1. If there is a cardiac history or potential for arrhythmia, correct if < 3. Sodium phosphate can be used.
4. Acidosis – No indication for bicarb unless the pH is ≤ 6.9 or if potassium > 6.4 mEq/L.
a. 100 mEq sodium bicarbonate in 400 mL of water.
b. Keep in mind that bicarb administration can cause hypokalemia or worsen it.
Monitoring includes….
- Q1h glucose checks
- Q2h metabolic panel
- Q2h VBG
Resolution of DKA and HHS
What we look for…
- Normalization of anion gap (<12)
- Absence of serum beta hydroxybuyterate level.
- Metal lucidity in HHS and plasma osmolality < 315
- Drop in glucose levels to 250 to 200 mg/dL
- Tolerance to PO diet.
CONVERSION TO SUBCUTANEOUS INSULIN
Only initiate subcutaneous insulin if the patient is able to eat and the above criteria regarding resolution of ketoacidosis is met.
HHS
1. Overlap 2 hours of insulin gtt when serum glucose reaches 250 to 300 mg/dL
DKA
1. Overlap 2 hours of insulin gtt when serum glucose reaches 200 mg/dL
2. In addition two of the following must be met
a. Anion gap < 12
b. Bicarb ≥ 15
c. Venous pH > 7.30
References:
1. Up to Date has the latest and best information
2. SAMC order set for DKA
3. Dr. Michael Moya's DKA Handout
Inpatient Diabetes Guidelines
- Type 1 DM: autoimmune. Patients require exogenous insulin to prevent DKA.
- Type 2 DM: insulin resistance and a relative insulin deficiency. Treatment may be with diet, exercise, oral meds, injectable meds, and/or insulin. With severe insulin deficiency, patients also develop DKA.
Basal: insulin needed even when the patient is not eating (to control gluconeogenesis).
- Use glargine (q24, typically at bedtime, preferred for type 1), NPH (qHS or qAM+HS), detemir (BID or q24 for larger doses), or a continuous insulin infusion.
Nutritional: insulin to cover carbohydrate intake from food, dextrose in IVF, tube feeds, TPN.
- Use rapid-acting insulin (aspart, lispro, or glulisine) or short-acting insulin (regular).
Correctional: insulin given to bring a high blood glucose level down to target range (130-150 pre-meal and 180-200 before bedtime).
- Use rapid-acting insulin (aspart, lispro, or glulisine) or short-acting insulin (regular).
- Remember that a patient with type 1 DM will always need exogenous basal insulin, even if NPO. Failure to do so will lead to DKA.
- Using correctional (“sliding scale”) insulin alone is acceptable for initial titration but should be reevaluated daily.
- Order a carbohydrate controlled meal plan. Each meal contains 60 to 75 grams of carbohydrates.
- Check blood glucose (BG) before meals and at bedtime, +/- at 2am (if suspect hypoglycemia) in a patient who is eating; check BG q 4 or q 6 hours in a patient who is NPO or is receiving continuous tube feeds or TPN.
- Involve the diabetes educator, nurse specialist and dietician.
- Supply glucose meter, lancets, test strips, syringes/pen needles, insulin, glucose tablets, and glucagon kit as discharge prescriptions, if needed. Health insurance dictates which types of supplies will be covered.
- Oral medications: often, oral diabetes medications are held upon admission to the hospital. Hospitalized patients have the potential for renal impairment and tissue hypoxia or need IV contrast, and these are all contraindications to metformin use. Sulfonylureas should generally be held upon admission if you anticipate NPO status due to high risk of hypoglycemia. If patient’s status improves and is reliably stable, consider restarting non-insulin medications.
- Nutritional insulin: regular is given within 30 min before meal, rapid-acting within 15 minutes before meal.
- Infection and glucocorticoids increase insulin needs; renal insufficiency decreases insulin needs.
- Total daily dose of insulin needed: type 1 patients require approximately 0.5 units/kg/day; type 2 patients vary in their insulin resistance and may require from 0.5 to 2 units/kg/day.
- BG <70 mg/dL: if patient is alert and taking PO, give 20 grams of oral fast-acting carbohydrate either as glucose tablets or 6 oz. fruit juice. If the patient cannot take PO, give 25 mL D50 IV push.
- Check BG every 15 minutes and repeat above treatment until BG is ≥100 mg/dL.
- The guidelines below may assist with initial determination and subsequent adjustment of insulin doses.
- Reevaluate insulin doses on a daily basis.
Correctional insulin (rapid or short acting): select between sensitive, average, or resistant based on BMI.
- Sensitive: BMI <20, or <50 units/day.
- Average: BMI 25-30, or 50-90 units/day.
- Resistant: BMI >30, or >90 units/day.
Nutritional insulin (rapid or short acting): continue with home nutritional doses, or can start based on meal consumption and titrate up as necessary. Remember to adjust and increase nutritional dosing as you observe daily insulin requirements. Example:
- Not eating: 0 units pre-meal dose.
- Eating <50% of meals: 1 unit pre-meal dose.
- Eating 50-75% of meals: 2 units pre-meal dose.
- Eating >75% of meals: 3 units pre-meal dose.
Insulin regimen for a patient controlled only with diet at home, but needing insulin in hospital:
- Day 1: order correctional insulin based on BMI (sensitive = BMI<25, average = BMI 25-30, resistant = BMI>30)
- Day 2: if BG pre-meals are >150 mg/dL, add nutritional insulin based on meal consumption (see above). Also, if AM fasting BG is >150 mg/dL, add bedtime basal insulin dosed 0.1 unit/kg.
- Day 3: adjust insulin doses based on BG pattern. Increase or decrease basal insulin based on AM fasting BG, and adjust nutritional insulin based on pre-meal BG levels. Approximately half the daily dose should be given as basal insulin, and the other half as divided doses with meals.
Insulin regimen for a patient on oral agent(s) at home:
- Day 1: start nutritional insulin based on meal consumption (see “Nutritional insulin” above). Also, order correctional insulin based on BMI (see “Correctional insulin” above).
- Day 2: if AM fasting BG is >150 mg/dL, add bedtime basal insulin dosed 0.1 unit/kg.
- Day 3: adjust insulin doses based on BG pattern. Increase or decrease basal insulin based on AM fasting BG, and adjust nutritional insulin based on pre-meal + bedtime BGs.
Insulin regimen for a patient on insulin at home:
- Assess home BG control, appetite, renal function, and risk for hypoglycemia.
- Basal insulin: continue home regimen if patient has been well-controlled at home, but consider giving only 80% of home dose to reduce the risk of in-hospital hypoglycemia. Or, start bedtime glargine or NPH dosed 0.2 units/kg.
- Nutritional insulin: order based on appetite, or consider pre-meal dosing of 0.2 units/kg divided by 3 for the dose at each meal.
- Correctional insulin: order based on total insulin dose or BMI.
Insulin regimen when a patient is made NPO for a procedure: a patient will always require his or her basal insulin, even while NPO, and should not become hypoglycemic if that basal is dosed appropriately. For safety purposes, however:
- The night before, give the usual dose of bedtime NPH, or decrease the usual dose of bedtime glargine by 25%.
- The morning of the procedure decrease the usual dose of morning NPH by 50%, or decrease the usual dose of morning glargine by 25%.
- Stop nutritional insulin (while patient is not eating), but continue the usual correctional insulin.
Insulin regimen for an ICU or surgical patient who is NPO: consider insulin infusion therapy. See your hospital-specific standardized protocol.
Insulin regimen for a patient starting continuous tube feeds:
- Consider insulin infusion therapy. See your hospital-specific standardized protocol.
- Estimate the tube feed formula’s 24-hour carbohydrate load (discuss with nutritionist).
- Estimate the total daily dose (TDD) of insulin, starting with 1 unit insulin for every 10 grams of carb.
- Basal need: divide the estimated TDD by 2 for the nightly glargine or total bid NPH dose.
- Nutritional insulin: divide the estimated TDD by 10 for the total nutritional dose, to be given q 4 hours (rapid acting insulin) or q 6 (regular insulin) hours.
- Correctional insulin: order based on total insulin dose or BMI.
Insulin regimen for a patient receiving TPN:
- Standard TPN often contains 25% glucose, which, if 100 ml/hour, yields 25 g glucose/hour; discuss with nutritionist to determine exact glucose load.
- Basal and nutritional insulin: adding insulin to the TPN can be a safe strategy, as the unexpected discontinuation of TPN will also mean the discontinuation of the insulin. Start with 0.1 unit per gram glucose.
- If the patient has previously required basal insulin, convert this dose to regular insulin and add to TPN (dose reduce to 80% for safety purposes).
- Correctional insulin: order based on BMI.
Insulin regimen to transition from an insulin infusion to subcutaneous insulin:
- Calculate the patient’s TDD of insulin, based on the most recent insulin infusion rate. For safety purposes, take 80% of that dose.
- Basal need: divide 80% of the TDD by half for basal insulin dose.
- Nutritional insulin: if the patient is eating, divide 80% of the TDD by half, and then split over three meals. If the patient is receiving tube feeds, divide 80% of the TDD by 10 for the nutritional dose, to be given q 4 hours (rapid acting) or 6 hours (regular).
- If the patient is not receiving nutrition, do not order nutritional insulin.
- Correctional insulin: order based on total insulin dose or BMI.
- Give the first basal insulin SQ injection 1-2 hours before the infusion is discontinued. If the transition is being made in the morning, consider using a one-time AM NPH injection or ½ of daily glargine dose to bridge until bedtime glargine or NPH begins.
Insulin regimen for a patient receiving steroids:
- Glucocorticoids will dramatically increase postprandial BG levels. Often, BG levels are very high during the day while steroids are active, then lower overnight.
- Anticipate post-prandial hyperglycemia by increasing the nutritional insulin doses.
- With glucocorticoids, give only 25% of TDD as basal insulin and 75% as pre-meal insulin.
- There are no validated formulas for making these adjustments, but the following are generally accepted rules of thumb.
- Basal insulin: adjusted based on fasting glucose (FBG) levels. For example:
- If FBG <140, no change.
- If FBG 141-160, increase basal dose by 2-3 units.
- If FBG 161-180, increase basal dose by 4-5 units.
- If FBG 181-200, increase basal dose by 6-7 units.
- If FBG >200, increase basal dose by 8 units.
- With this approach, the basal insulin can be titrated up to the patient’s actual requirement relatively quickly.
- Nutritional insulin: the adequacy of the nutritional insulin dose is based on the glucose level prior to the next meal. For example, the glucose level just before lunch will indicate whether the insulin given at breakfast was appropriate. A simple approach is as follows:
- If there was no significant change in the glucose level from before breakfast to before lunch, then the total dose of insulin the patient received at breakfast (nutritional plus correctional) should be used as the nutritional dose for breakfast the next day.
- If there was a significant increase in the glucose level from before breakfast to before lunch, then the total dose of insulin the patient received at breakfast (nutritional plus correctional) should be increased and should become the nutritional dose for breakfast the next day.
- If the glucose level before breakfast was high, and the glucose level at lunch was at goal, then no change in the nutritional dose will be required for the next day.
- Finally, no matter what the glucose level was at breakfast, if the glucose level after breakfast or before lunch was low, then the breakfast nutritional dose should be decreased for the next day.
Hypothyroidism
Definition
Primary Hypothyroidism: High TSH and Low T4
Secondary (central) Hypothyroidism: Low T4 and TSH that is low
Subclinical Hypothyroidism: High TSG with normal T4
Myxedema coma: severe hypothyroidism causing multi-organ dysfunction. A medical emergency with a high mortality rate
Presentation
Early: Usually asymptomatic, but may have fatigue, weight gain, cold intolerance, menorrhagia or amenorrhea, constipation, dry skin, thin hair, delayed DTR, diastolic HTN and hyperlipidemia
Late: Slow speech, brawny edema, hoarseness, loss of outer third of eyebrows, puffy face/eyelids, thickened tongue, myxedema, bradycardia, hypotension, and hypothermia
Myxedema coma: Endocrine emergency. Can present with AMS, hypothermia, hypoventilation, hyponatremia, hypoxia, hypercapnia, hypotension, convulsion, confusion, lethargy and coma.
Management
Levothyroxine: Full replacement is approx 1.6mcg/kg/day. Patient not requiring full replacement can be started on lower dose
Monitoring and dose adjustment based on TSH every 4-8 weeks until stable dose achieved
Pregnancy: Goal TSH varies by trimester, consultation with endocrinology is indicated
Elderly with CAD or high risk CAD, long standing untreated hypothyroidism: Start levothyroxine 25mcg/day
Subclinical hypothyroidism: Treatment generally not necessary unless TSH is >10, anti TPO positive, presence of a goiter, pregnancy or other compelling complication. Typically lower doses of levothyroxine are needed. Start with 15-50mcg. Follow up in 4-8 weeks of treatment initiation.
Thyroid Cancer: Patient who had total thyroidectomy for thyroid cancer need higher doses of thyroid hormone to suppress TSH
Myexedema coma:
- Immediate endocrine consult to help guide therapy,
- draw cortisol level first and administer steroid (hydrocortisone 50-100mg q6-8h) until adrenal insufficiency can be ruled out. Thyroid hormone therapy can increase cortisol clearance, precipitating adrenal insuffiency.
- Thyroid replacement: 200-400mcg IV load followed by 50-100mcg IV daily. Consider lower IV load doses in elderly patients or patient with cardiac conditions
https://pubmed.ncbi.nlm.nih.gov/23246686/
Hospitalist handbook
Hyperthyroidism
Symptoms and signs
- Signs of hypermetabolic state: restlessness, tachycardia, diaphoresis, hyper-defecation, weight loss, palpitation
- Apathetic hyperthyrodism: elderly patients often don't have classic symptoms, but may present with lethargy, weight loss, SOB and afib
- Thyroid Storm: Fever, delirium, stupor, coma, tachycardia, arrhytmias, CHF, vomiting/diarrhea, hepatic failure
Work up
- TSH suppressed (except in pituitary disease), T4 and/or T3 increased
- ESR can be increased in subacute thyroiditis
- Anti TPO Ab often positive in silent thyroiditis
- Radioactive iodine uptake can be useful to differentiate between causes (contraindicated in pregnant patients): diffuse high uptake in graves', focal high uptake with toxic nodule, very low uptake in subacute thyroiditis.
- Burch-Wartofsky Point Scale (BWPS) is a scoring system to help identify thyroid storm
Management
Medical Therapy
Symptom Management: Propanolol to control symptoms and tachycardia (blocks adrenergic effects and peripheral conversion of T4 to T3). Beta blockade can be stopped once anti-thyroid treatment takes effect.
Inhibition of hormone synthesis: Methimazole or PTU. Methimazole is generally preferred due to better side effect profile (PTU preferred in pregnancy). Obtain baseline CBC and LFT's
Definitive therapy: Radioactive iodine ablation
Thyroid storm
- Consult endocrinology
- Supportive therapy with IVF, Oxygen and acetaminophen, likely ICU
- Avoid ASA as it can displace T4 from TBG
- Immediately start PTU 200-300mg PO q406hr
- Follow with saturated solution of potassium iodide to inhibit conversion of T4 to T3
- Consider propanolol 60-80mg PO q4-6hr to control tachycardia (caution in Heart Failure)
- Consider hydrocortisone 50-100mg IV q6-8hrs x48 hrs (blocks conversion of T4-T3)
Hospitalist Handbook
Gastroenterology
GI bleed
Etiology
- The site of bleeding is only suggested by the patient’s presentation and physical examination.
- Stool can turn black (melena) with as little as 50-100 cc of upper GI bleeding
Pre-endoscopic clinical risk stratification
Clinical judgment always comes first.
- Assess the following features, based in part upon Rockall scale, BLEED criteria and Glasgow-Blatchford score.
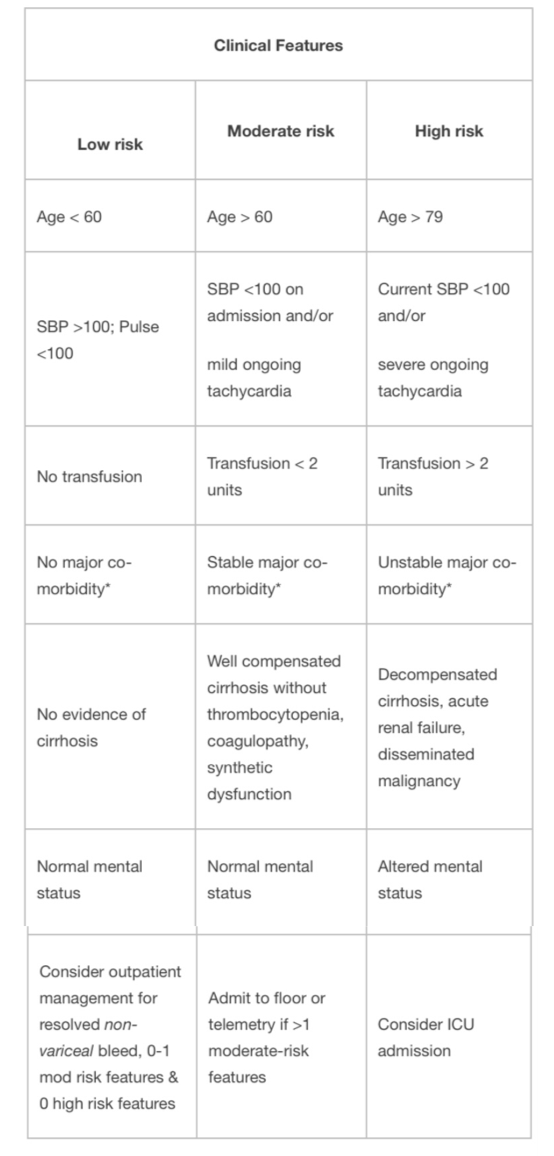
*Major co-morbidity defined as CAD, CHF, renal failure, liver disease, sepsis, disseminated malignancy, altered
mental status, pneumonia, COPD, asthma.
- Use clinical risk to determine urgency of endoscopy and level of care required.
- Absolute indications for ICU admission:
- Shock
- Orthostasis
- Acute HCT decrease by >6%
- Transfusion requirements >2units pRBCs
- Active bleeding – ongoing hematemesis, bright red blood per NGT, hematochezia
- Most deaths are secondary to respiratory, cardiovascular, infectious, and renal complications associated with bleeding, not from exsanguination.
Evaluation
- Risk factors/Hx: NSAID use, alcohol use, liver disease/varices, severe retching, h/o GI bleed, past endoscopy, prior abdominal surgery, aortic aneurysms/grafts, trauma, coagulopathy, anticoagulation, malignancy
- Physical Exam:
- VS (with orthostatics)
- Rectal – note the color/consistency of stool (black/tarry = melena; bright red blood = hematochezia), palpable masses, external anal findings (e.g., hemorrhoids, fissures), smear stool on paper towel to see true color/content
- Guaiac testing is not useful to determine inpatient management
- Abdominal mass, peritoneal signs
- Stigmata of ESLD (asterixis, ascites, spiders, palmar erythema, caput, jaundice, testicular atrophy, gynecomastia)
- HEENT: epistaxis, telangiectasias (hereditary hemorrhagic telangiectasias, EtOH.)
- NG lavage is not required for upper GI bleeding patients. Endoscopist may use in certain patients to triage the timing of endoscopy but should not be placed routinely. It can be helpful in severe hematochezia patients to differentiate brisk upper GI bleed from lower GI bleeding.
- Coagulopathy and varices are not contraindications to NG tube placement.
- Note amount of aspirate obtained, the quality of the aspirate, and amount of saline lavage that is required to clear it.
- The lack of blood in the NG aspirate does not rule out an upper GI bleed as it may have only sampled gastric content and bleed may be duodenal
- Bile in the aspirate may confirm placement beyond the pylorus
- Low threshold to get KUB if peritoneal signs or abdominal distension. CT is more sensitive for free air, perforation, or ischemia.
- ECG for patients with a history of CAD or age > 45.
Management
Evaluation and Stabilization:
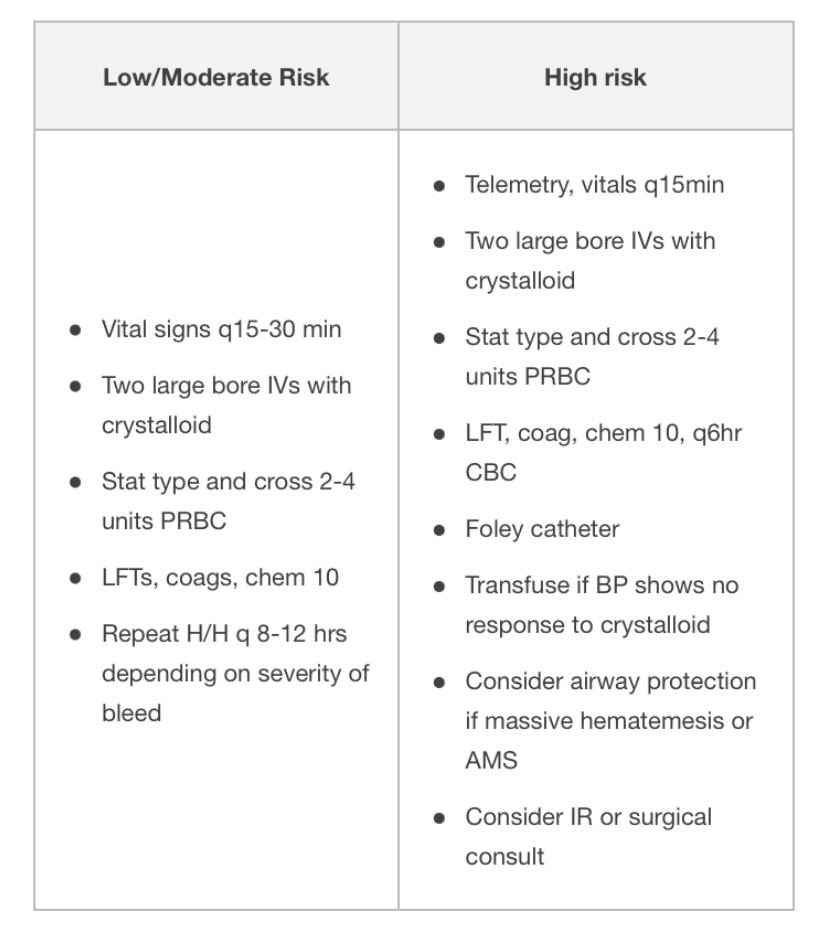
Common Management of Upper and Lower GI bleed
- NPO until cleared by GI
- Volume resuscitate with crystalloid.
- 2 large bore (16g or larger) PIVs.
- Consider cordis or rapid infusion catheter instead of triple lumen for central access.
- Most recent studies support restrictive transfusion strategies (goal Hg>7), though may consider goal of Hg>8 for patients with CAD.
- Protonix (bolus 80mg IV x 1 à 8mg/hr IV gtt)
- Reduces mortality in lesions subsequently seen to have high-risk stigmata for rebleed, reduces rebleeding after endoscopy, length of stay, and need for transfusion in patients with high-risk ulcer
- PPI before endoscopy: no difference in mortality, re-bleed rate, or need for surgery than if given after endoscopy, but decreases rate of high-risk stigmata of re-bleeding and need for subsequent endoscopic therapy
- Check H. pylori (serologies, endoscopic biopsy, stool antigen) and treat if present.
- H. Pylori diagnostic testing has higher false-negative rates in setting of bleeding (or PPI use.) Repeat if negative in setting of acute bleeding and clinical suspicion is high.
- Consider FFP, vitamin K if INR > 1.5, prothrombin complex concentrate (such as Kcentra), DDAVP (0.3 mcg/kg IV q12h x 2 doses) if uremic bleeding, and platelets if platelet count < 50. In ESLD patients, also order fibrinogen & replete with cryoprecipitate to >100.
- Consider massive transfusion protocol if hemodynamically unstable/requiring large amount of blood products.
- Complications of massive transfusion:
- metabolic alkalosis (2/2 citrate metabolism) in setting of renal impairment
- hypokalemia (precipitated by alkalosis)
- hypocalcemia (due to citrate binding)
- hypothermia
- hyperkalemia (particularly with older blood products)
- Avoid NSAIDs, ASA, anticoagulants
- Surgery consult if recent surgical procedure or rebleeding (>6u pRBC)
- Re-bleeding:
- Preferred treatment is repeat endoscopic therapy
- If patient has persistent bleeding after endoscopy, consider CT angiogram or IR embolization. For uncontrolled bleeding requiring >6u pRBC there is no significant difference (rates of re-bleeding, subsequent therapy, or mortality) for IR embolization vs. surgical intervention.
- Other diagnostic modalities (discuss with GI first)
- Tagged RBC scan (can detect bleed rate >0.1cc/min, localizes bleeding to area of abdomen but variable localization to portion of intestinal tract, can re-scan several times over 24-48h after tagged RBC administration for intermittent bleeding). If positive, consider IR embolization.
- CT (mesenteric) angiography (requires >1 cc/min.)
Specific management for suspected variceal bleed
- Goal hemoglobin > 7, plt >50, INR <1.5. More aggressive resuscitation may result in higher rates of re-bleed due to increase in portal pressures, particularly if Hb > 9.
- Octreotide 100 mcg bolus then 50 mcg/hr x 72 hours (constrict splanchnic circulation.)
- Discontinue PPI drip after endoscopy if there is no ulcer.
- Ceftriaxone (1gm q24 hrs x 5 days): reduces variceal re-bleeding, infection, and mortality in patients with cirrhosis +/- ascites.
- Endoscopy fails to control bleeding in ~10-20% patients.
- For persistent bleeding or re-bleed:
- Repeat endoscopic therapy
- Balloon tamponade (e.g. Sengstaken-Blakemore,tube): 50% rate of re-bleed upon balloon deflation, other complications including esophageal necrosis, rupture.
- TIPS
- Surgery
- Beta blockers: use in patients with proven variceal bleeds after the acute bleed has resolved and s/p octreotide x 72 hours. Nonspecific beta blockers (propranolol, nadolol) can be used as secondary prophylaxis against variceal re-bleeding .
- Titrate to a dose that lowers the baseline heart rate by 25% or to goal heart rate 55-60, as tolerated by the patient (15-30% of patients won’t tolerate due to low blood pressure.)
- Arrange for GI follow-up (endoscopy) for serial banding.
Endoscopy
- Diagnostic and therapeutic, as well as prognostic
- Correction of anticoagulation should not delay endoscopy
The following are endoscopic findings that a GI consultant uses to further risk stratify patients:
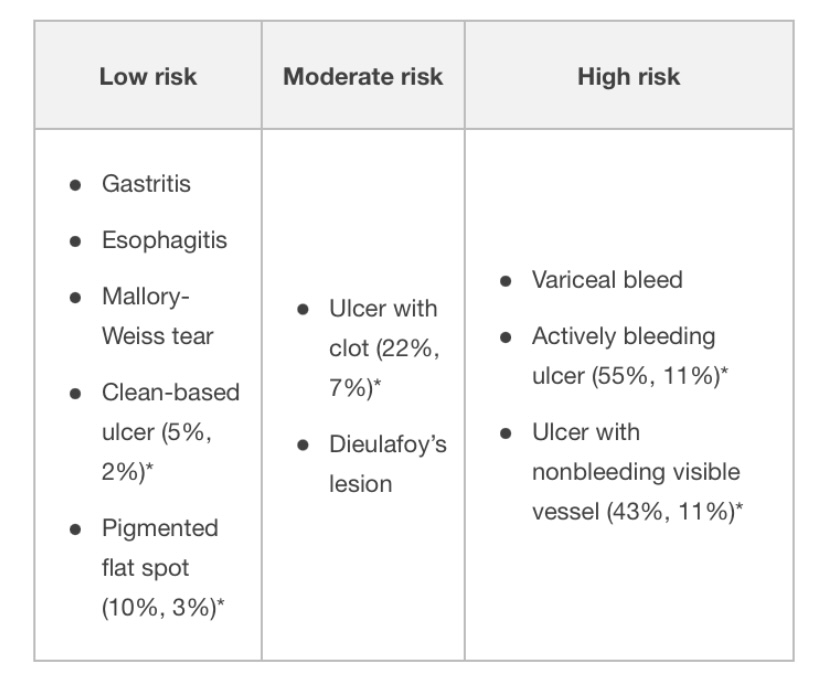
* Risk of (rebleeding, mortality rate)
- Length of observation for re-bleeding after endoscopy depends on endoscopic and clinical risk criteria. Rapid post-endoscopy discharge is reasonable for some patients with low-risk endoscopic findings, but discuss with GI first.
Key points
- Melena requires as little as 50-100 cc of blood and usually signals upper GI bleed, but can occur with light colonic bleeding with a slow transit time
- Most deaths occur from respiratory, cardiovascular, infectious, and renal complications associated with bleeding, and not exsanguination.
- NG tube lavage is not routinely required in all GI bleed patients
- The lack of blood in the NG aspirate does not rule out an upper GI bleed
Reference: Hospitalist Handook
Ascites
Definition
- Accumulation of peritoneal fluid
Symptoms
- Abdominal Distention and discomfort
- Anorexia
- Nausea
- Early satiety
- Heartburn (Gastroesophageal Reflux)
- Flank Pain
- Respiratory distress
Signs
- Umbilicus may evert
- Bulging flanks with the patient lying supine
- Fluid Wave Test
- Shifting Dullness Test
- Puddle Sign
Most common etiologies
- Cirrhosis (Cirrhotic Ascites): 85% of cases
- Cancer (Malignant Ascites)
- Congestive Heart Failure
- Tuberculosis
Labs
- Diagnostic abdominal Paracentesis
- Ascites Fluid: Cell Count with Differential, albumin/protein concentration and ascitic fluid inoculation in blood culture bottles, Serum Ascites albumin gradient (SAAG), cytology
Ascites fluid assorted labs
Serum
- CBC, CMP (electrolyte imbalance, LFT, hepatorenal), BNP, PT, aPTT, INR,
Imaging
Medication Management
- Spironolactone and
- Thiazide or Loop Diuretic (diuretic dosage should be adjusted to a daily weight loss of no more than 500 g/day in patients without peripheral edema and 1 kg/day in patients with peripheral edema)
- Electrolyte correction
- Consider Hepatic encephalopathy management
- Paracentesis (consider Albumin)
- Antibiotic (therapeutic/prophylaxis for SBP)
- Electrolyte replacement, restriction of daily sodium intake to 80–120 mmol
Executive summary of recommendations
-
Diagnostic paracentesis in new- onset ascites
-
1.1. A diagnostic paracentesis is recommended in all patients with new-onset ascites. (Quality of evidence: moderate; Recommendation: strong)
-
1.2. The initial ascitic fluid analysis should include total protein concentration and calculation of the serum ascites albumin gradient (SAAG). (Quality of evidence: moderate; Recommendation: strong)
-
1.3. Ascites fluid analysis for cytology, amylase, brain natriuretic peptide (BNP), and adenosine deaminase should be considered based on the pretest probability of specific diagnosis (Quality of evidence: moderate; Recommendation: weak)
-
-
Spontaneous bacterial peritonitis
-
2.1. Diagnostic paracentesis should be carried out without delay to rule out spontaneous bacterial peritonitis SBP) in all cirrhotic patients with ascites on hospital admission. (Quality of evidence: moderate; Recommendation: strong)
-
2.2. A diagnostic paracentesis should be performed in patients with GI bleeding, shock, fever or other signs of systemic inflammation, gastrointestinal symptoms, hepatic encephalopathy, and in patients with worsening liver or renal function. (Quality of evidence: moderate; Recommendation: strong)
-
2.3. Ascitic neutrophil >250/mm3 count remains the gold standard for the diagnosis of SBP and this can be performed either by manual microscopy or using automated counts, based on flow cytometry for counting and differentiating cells. (Quality of evidence: moderate; Recommendation: strong)
-
2.4. Ascitic fluid culture with bedside inoculation of blood culture bottles should be performed to guide the choice of antibiotic treatment when SBP is suspected. (Quality of evidence: moderate; Recommendation: strong)
-
2.5. Immediate empirical antibiotic therapy should be determined with due consideration of the context of SBP (community-acquired or healthcare-associated), the severity of the infection, and the local bacterial resistance profile. Cefotaxime has been widely studied, but the choice of antibiotic should be guided by local resistance patterns and protocol. (Quality of evidence: moderate; Recommendation: strong)
-
2.6. A second diagnostic paracentesis at 48 hours from the start of treatment to check the efficacy of antibiotic therapy should be considered in those who have an apparently inadequate response or where secondary bacterial peritonitis is suspected. (Quality of evidence: low; Recommendation: weak)
-
2.7. Patients presenting with gastrointestinal bleeding and underlying ascites due to cirrhosis should receive prophylactic antibiotic treatment (cefotaxime has been widely studied but the antibiotic should be chosen based on local data) to prevent the development of SBP. (Quality of evidence: strong; Recommendation: strong)
-
2.8. Patients who have recovered from an episode of SBP should be considered for treatment with norfloxacin (400 mg once daily), ciprofloxacin (500 mg once daily, orally), or co-trimoxazole (800 mg sulfamethoxazole and 160 mg trimethoprim daily, orally) to prevent a further episode of SBP. (Quality of evidence: low; Recommendation: weak)
-
2.9. Primary prophylaxis should be offered to patients considered at high risk, as defined by an ascitic protein count <1.5 g/dL. However, it is important that the potential risks and benefits and existing uncertainties are communicated to patients. (Quality of evidence: low; Recommendation: weak)
-
-
Dietary salt restriction
-
3.1. Patients with cirrhosis and ascites should have a moderately salt-restricted diet with a daily salt intake of no more than 5–6.5 g (87–113 mmol sodium). This translates to a no added salt diet with avoidance of precooked meals. (Quality of evidence: moderate; Recommendation: strong)
-
3.2. Patients with cirrhosis and ascites should receive nutritional counseling on the sodium content in the diet. (Quality of evidence: weak; Recommendation: strong)
-
-
Diuretics
-
4.1. In patients with the first presentation of moderate ascites, spironolactone monotherapy (starting dose 100 mg, increased to 400 mg) is reasonable. In those with recurrent severe ascites, and if faster diuresis is needed (for example, if the patient is hospitalized), combination therapy with spironolactone (starting dose 100 mg, increased to 400 mg) and furosemide (starting dose 40 mg, increased to 160 mg) is recommended. (Quality of evidence: moderate; Recommendation: strong)
-
4.2. All patients initiating diuretics should be monitored for adverse events. Almost half of those with adverse events require diuretic discontinuation or dose reduction. (Quality of evidence: low; Recommendation: weak)
-
4.3. Hypovolaemic hyponatremia during diuretic therapy should be managed by discontinuation of diuretics and expansion of plasma volume with normal saline. (Quality of evidence: low; Recommendation: weak)
-
4.4. Fluid restriction to 1–1.5 L/day should be reserved for those who are clinically hypervolaemic with severe hyponatremia (serum sodium <125 mmol/L). (Quality of evidence: low; Recommendation: weak)
-
4.5. Hypertonic sodium chloride (3%) administration should be reserved for those who are severely symptomatic with acute hyponatremia. Serum sodium should be slowly corrected. (Quality of evidence: low; Recommendation: weak)
-
4.6. It may be appropriate to consider the use of midodrine in refractory ascites on a case-by-case basis. (Quality of evidence: low; Recommendation: weak)
-
-
Large volume paracentesis (LVP)
-
5.1. Patients should give informed consent for a therapeutic or diagnostic paracentesis. (Quality of evidence: low; Recommendation: strong)
-
5.2. Ultrasound guidance should be considered when available during LVP to reduce the risk of adverse events (Quality of evidence: low; Recommendation: weak)
-
5.3. Routine measurement of the prothrombin time and platelet count before therapeutic or diagnostic paracentesis and infusion of blood products are not recommended. (Quality of evidence: moderate; Recommendation: strong)
-
-
Use of human albumin solution (HAS)
-
6.1. Albumin (as 20% or 25% solution) should be infused after paracentesis of >5 L is completed at a dose of 8 g albumin/L of ascites removed. (Quality of evidence: high; Recommendation: strong)
-
6.2. Albumin (as 20% or 25% solution) can be considered after paracentesis of <5 L at a dose of 8 g albumin/L of ascites removed in patients with ACLF or high risk of post-paracentesis acute kidney injury. (Quality of evidence: low; Recommendation: weak)
-
6.3. In patients with SBP and increased serum creatinine or rising serum creatinine, infusion of 1.5 g albumin/kg within 6 hours of diagnosis, followed by 1 g/kg on day 3, is recommended. (Quality of evidence: low; Recommendation: weak)
-
-
Transjugular intrahepatic portosystemic shunt (TIPSS)
-
7.1. TIPSS should be considered in patients with refractory ascites. (Quality of evidence: high; Recommendation: strong)
-
7.2. Caution is required if considering TIPSS in patients with age >70 years, serum bilirubin >50 µmol/L, platelet count <75×109/L, a model for end-stage liver disease (MELD) score ≥18, current hepatic encephalopathy, active infection or hepatorenal syndrome. (Quality of evidence: moderate; Recommendation: strong)
-
-
Umbilical hernia
-
8.1. Suitability and timing of surgical repair of umbilical hernia should be considered in discussion with the patient and multidisciplinary team involving physicians, surgeons, and anesthetists. (Quality of evidence: low; Recommendation: strong)
-
-
Hepatic hydrothorax (HH)
-
9.1. TIPSS should be considered in patients with HH after discussion with the multidisciplinary team. (Quality of evidence: low; Recommendation: strong)
-
9.2. In patients with HH who are not undergoing a TIPSS and/or a liver transplant evaluation, alternative palliative interventions should be considered. (Quality of evidence: low; Recommendation: strong)
-
-
Non-selective beta-blockers (NSBB) and ascites
-
10.1. Refractory ascites should not be viewed as a contraindication to NSBB. (Quality of evidence: moderate; Recommendation: strong)
-
10.2. Patients with refractory ascites who are taking NSBB should be monitored closely, and dose reduction or discontinuation may be appropriate in those who develop hypotension or acute/progressive renal dysfunction. (Quality of evidence: moderate; Recommendation: strong)
-
Reference
- Pedersen JS, Bendtsen F, Møller S. Management of cirrhotic ascites. Ther Adv Chronic Dis. 2015;6(3):124-137. doi:10.1177/2040622315580069
- , et al Guidelines on the management of ascites in cirrhosis
SBP
Definition
SBP is a bacterial infection of the ascitic fluid.
Diagnosis:
PMN count >= 250 cells/mm3 OR ascitic fluid WBC >= 500 cells/mm3 with a positive fluid culture.
Diagnostic clinical signs: New onset fever, confusion or abdominal pain, hepatic encephalopathy, vomiting, diarrhea.
Diagnosis of Culture-negative neutrocytic ascites: PMN count >= 250 cells/mm3 with a negative fluid culture (subtract 1 PMH for every 250 RBCs).
Pathogens causing SBP: Common organisms are E. coli, Klebsiella pneumoniae, Enterobacteriaceae, Streptococcus pneumoniae, and Enterococcus.
Patients with Cirrhosis: Cirrhotic patients can also get secondary bacterial peritonitis, which usually requires surgical intervention. One should suspect secondary peritonitis with perforation if the ascitic fluid meets 2 or more of the following: Total WBC >10,000, Total protein > 1 g/dl, Glucose < 50 mg/dl OR LDH > 225 milliunits/ml (or higher than upper normal for serum). One should also be suspicious if multiple organisms are cultured or if there is a failure to improve after 48 hours of standard therapy.
Risk Factors for SPB: Severe liver disease, GI hemorrhage, Prior SBP, Ascitic fluid protein <= 1 g/dl.
Diagnosis of SBP: Abdominal paracentesis, send fluid for cell count and differential and send fluid directly in the culture bottles.
Treatment for SBP:
Start antibiotic therapy as soon as the diagnosis of SBP is made based on fluid PMN count OR earlier if clinically indicated.
Use a third-generation cephalosporin (cefotaxime or a similar third generation cephalosporin) HIGH dose 2gm every 8 hours for 5 days.
Any person with cirrhosis and ascites who has signs or symptoms concerning for SBP should be treated with antibiotic therapy regardless of ascites fluid PMN count.
Antibiotic Prophylaxis for SBP: Prophylaxis should be given to persons with cirrhosis with a prior history of SBP or acute GI bleeding and should be considered in those who have renal or hepatic dysfunction if total ascitic fluid protein is less than 1.5g/dL.
Primary and Secondary SBP Prophylaxis: Ciprofloxacin 500 mg daily or trimethoprim-sulfamethoxazole one double strength tablet daily. If patient has cirrhosis and acute GI hemorrhage, IV ceftriaxone 1 gram daily is recommended for a total duration of 7 days.
Acute Pancreatitis
Definition
indicates inflammation of the pancreas.
Acute pancreatitis: results from the leakage of pancreatic enzymes into pancreatic tissue, leading to autodigestion.
Chronic pancreatitis: causes are varied and lead to destruction of the pancreatic tissue. Patients may present with pain and/or weight loss due to fat and protein malabsorption.
Clinical Symptoms of Acute Pancreatitis:
sudden onset of epigastric pain that lasts for hours to days and radiates to the back, nausea and vomiting, sweating, weakness, and anxiety. The patient often feels better when sitting up and leaning forward.
Physical examination findings of Acute Pancreatitis:
The patient may be febrile, tachycardic, tachypneic, and hypotensive. The skin of the periumbilical area may be discolored (Cullen’s sign). Flank ecchymoses (Grey Turner’s sign) may be present. The abdomen may have mild distention (because of ileus). Upper abdominal and epigastric tenderness (usually without rebound or rigidity) is often present.
Laboratory findings of Acute Pancreatitis:
Elevated serum amylase and lipase. Blood amylase or lipase levels are typically elevated three times the normal level during acute pancreatitis.
Other findings may include leukocytosis (12,000–15,000/μL), hypoalbuminemia, hyperglycemia, and elevated aspartate aminotransferase (AST, SGOT), alkaline phosphatase, and bilirubin.
Imaging for Suspected Acute Pancreatitis [but not necessary]:
CT ABDOMEN- PELVIS.
Causes of Acute Pancreatitis:
Biliary stones, Alcohol abuse, Drugs, Hyperlipidemia or Hypercalcemia, Idiopathic or Infectious, Trauma, Surgery (after endoscopic retrograde cholangiopancreatography [ERCP], intra-abdominal surgery) or Scorpion sting.
- Biliary stonesare the most common cause of acute pancreatitis in hospitalized patients.
- Alcohol abuseis the most common cause of pancreatitis overall in the United States.
- Many drugs can cause acute pancreatitis: thiazide diuretics, sulfa antibiotics, pentamidine, and some antiretroviral agents.
- Hyperlipidemia (types I, IV, V).Pancreatitis usually does not occur in hyperlipidemic patients until their serum triglyceride level exceeds 1000 mg/dL.
- Idiopathic causes: possibly due to pancreas divisum (a congenital defect), autoimmune pancreatitis, or microlithiasis as the cause. Pancreatic malignancy can also cause acute pancreatitis.
- Infectious etiologiesinclude mumps, cytomegalovirus (CMV), human immunodeficiency virus (HIV), and infections caused by Escherichia coli.
- Blunt, rather than penetrating, trauma. Blunt trauma may cause ductal disruption, leakage of pancreatic enzymes, and autodigestion of the pancreas leading to pancreatitis.
- Surgical: Postsurgical pancreatitis in patients undergoing ERCP.
- Scorpion stings: Scorpion stings are a common cause of pancreatitis in the Caribbean islands of Trinidad and Tobago.
Ranson’s criteria are used to assess severity and prognosis.
Ranson’s criteria are assessed at admission and during the initial 48 hours.
Ranson’s Criteria During the Initial 48 Hours. Ranson’s greater than 3 is SEVERE.
Base deficit >4 mEq/L
Calcium <8 mg/dL
Hematocrit decrease >10%
Sequestration of fluid >6 L
Oxygen <60 mm Hg
Blood urea nitrogen (BUN) increase of >5 mg/dL
As the number of criteria met increases, so does the mortality rate.
Treatment of Acute Pancreatitis:
- Treatment is primarily supportive and includes bowel rest, aggressive volume resuscitation, pain control, and management of respiratory distress and renal failure.
- Early feeding of patients with pancreatitis (as opposed to prolonged bowel rest) may be associated with improved outcomes.
- Nasogastric tubes are used for gastric decompression in patients with persistent vomiting.
- If gallstones are thought to be the cause, ERCP may be indicated.
- Cholecystectomy should only be considered after the patient recovers from the acute episode.
Complications of Acute Pancreatitis:
- Pancreatic abscess: should be suspected if the patient worsens after initial improvement. Persistent pain and fever are clues to the occurrence of an abscess. Re-image the patient with a CT scan.
- Pancreatic pseudocyst: occurs in 10%–20% of patients.
- Renal failure and respiratory failure are the two most common systemic complications and can be life-threatening.
Alcoholic Hepatitis
3 Histological Stages
- Simple steatosis (usually reversible w/ abstinence in 4-6 wks)
- Steatohepatitis (steatosis + neutrophil infiltration + Mallory-Denk bodies)
- Steato-fibrosis (extreme is cirrhosis)
MELD SCORE [calculate with mdcalc]
Model for End-Stage Liver Disease (MELD) score is a prognostic scoring system used to predict 3-month mortality due to liver disease
MELD scores range from 6 to 40; the higher the score, the higher the 3-month mortality related to liver disease
MDF SCORE [calculate with mdcalc]
Maddrey Discriminant Function (MDF) score is a measure of disease prognosis in alcoholic hepatitis (AH) used to identify patients at highest risk of mortality and determine the need for initiation of pharmacologic treatment.
An acute inflammatory syndrome that develops in the setting of chronic liver inflammation w/ alcohol use.
Risk Factors
Amount of alcohol, duration of alcohol use (>5-10 yrs for cirrhosis), gender (F>M), ethnicity (↑risk in AA & Hispanics), HCV (>30x ↑risk for cirrhosis), genetic mutations (PNLPA3) and obesity
Clinical Presentation
Hepatomegaly, jaundice, ascites, encephalopathy and fever.
Of note: alcohol related hepatitis can lead to portal HTN and varices and ascites in the absence of cirrhosis due to hepatic swelling and portal venous obstruction.
Diagnosis
- Often cholestatic LFTs (↑alk phos) with elevated AST & ALT (usually <300), typically in >2:1 ratio).
- ALT can be normal if vitamin B6 deficiency.
- ↑WBC
Treatment for Alcohol Related Hepatitis
- If MDF ≥ 32 (Or MELD >20) and/or presence of encephalopathy commence steroids: prednisolone 40mg/d for 4 weeks +/- taper x 2-4 weeks. Adding NAC may be beneficial, but ask for GI input before starting. Consider pentoxyfylline if steroids are contraindicated. Consult hepatology for consideration of early liver transplant if appropriate.
- Contraindications to prednisolone: active infection, chronic HBV/HCV, GIB, pancreatitis, renal failure.
- Lille Score: composite score of age, Cr, alb, PT, Tbili on day 0 and Tbili on day 7 of steroids. Calculate on day 7 to evaluate response to steroids; a score >0.56 indicates lack of response at 7 days → can discontinue steroids.
- Supportive therapy: monitor for infection, consider PPI/ H2RA, monitor for signs of HRS and avoid nephrotoxic drugs, hold beta blockers if MDF ≥ 32 due to incidence of AKI.
- Nutrition therapy: MVI, thiamine, folate, enteral feeding; nutrition independently decreases mortality.
- Only abstinence from alcohol and liver transplant are effective for long term treatment of alcohol related hepatitis. At discharge, patients should receive medication assisted therapy (acamprosate 666 mg TID, naltrexone 50mg QD, baclofen 5- 10mg TID, gabapentin 600mg TID)
Nausea
Nausea is the unpleasant sensation of about to vomit. This can occur alone or with vomiting. Many differentials are associated with nausea depending on patient's symptoms.
Always check patients electrolytes if they have been having severe vomiting and replete electrolytes if required. Suggestive labs could include BMP (checking electrolytes), UA (checking for ketones and specific gravity).
Treatment of nausea includes:
- Metoclopramide (Reglan) 10mg po/iv q4hr PRN
- Prochlorperazine (Compazine) 10mg po/im/iv q6hr
- Droperidol 0.625-1.25mg IV/IM q6hr PRN
- Lorazepam (Ativan) 0.5-2.0 mg po/iv q4-6hr PRN
Things to prevent nausea include:
- Ginger ale or chamomile tea to settle that stomach
- Avoiding caffeine that tends to upset stomach
- Drink lots of water and stay hydrated
- Eating small meals to allow your stomach to digest foods slowly
- Avoiding spicy, processed foods
Neuroleptic Malignant Syndrome can be caused by excessive use of Compazine or Droperidol (stop antiemetic and start Lorazepam 1-2mg IV 4-6hrs or Dantrolene 1-2.5 mg/kg IV with max dose of 10mg/kg/day).
Advise all patients that Antiemetics can cause drowsiness
Combination of anti-emetics will resolve patient's nausea if patient is unresponsive to a single medication.
Constipation
Check if patient has Bowel Obstruction before giving anything PO
Stool Softeners - Colace 100-250mg po qd or bid
Osmotic Laxatives
- MiraLAX 17gm daily
- Lactulose 30ml q4hr until bowel movement
- Milk of Magnesia 30ml to 60ml qd
Suppository - Dulcolax 10mg qd, mineral oil enema, fleet enema
Patients started on narcotics should be advised about constipation. Also patient's on chronic narcotics should be on bowel regimen to prevent constipation.
Hematology
Anemia
Anemia can be caused by many things but first we should get some basic labs such as CBC that will show MCV, and Reticulocyte count.
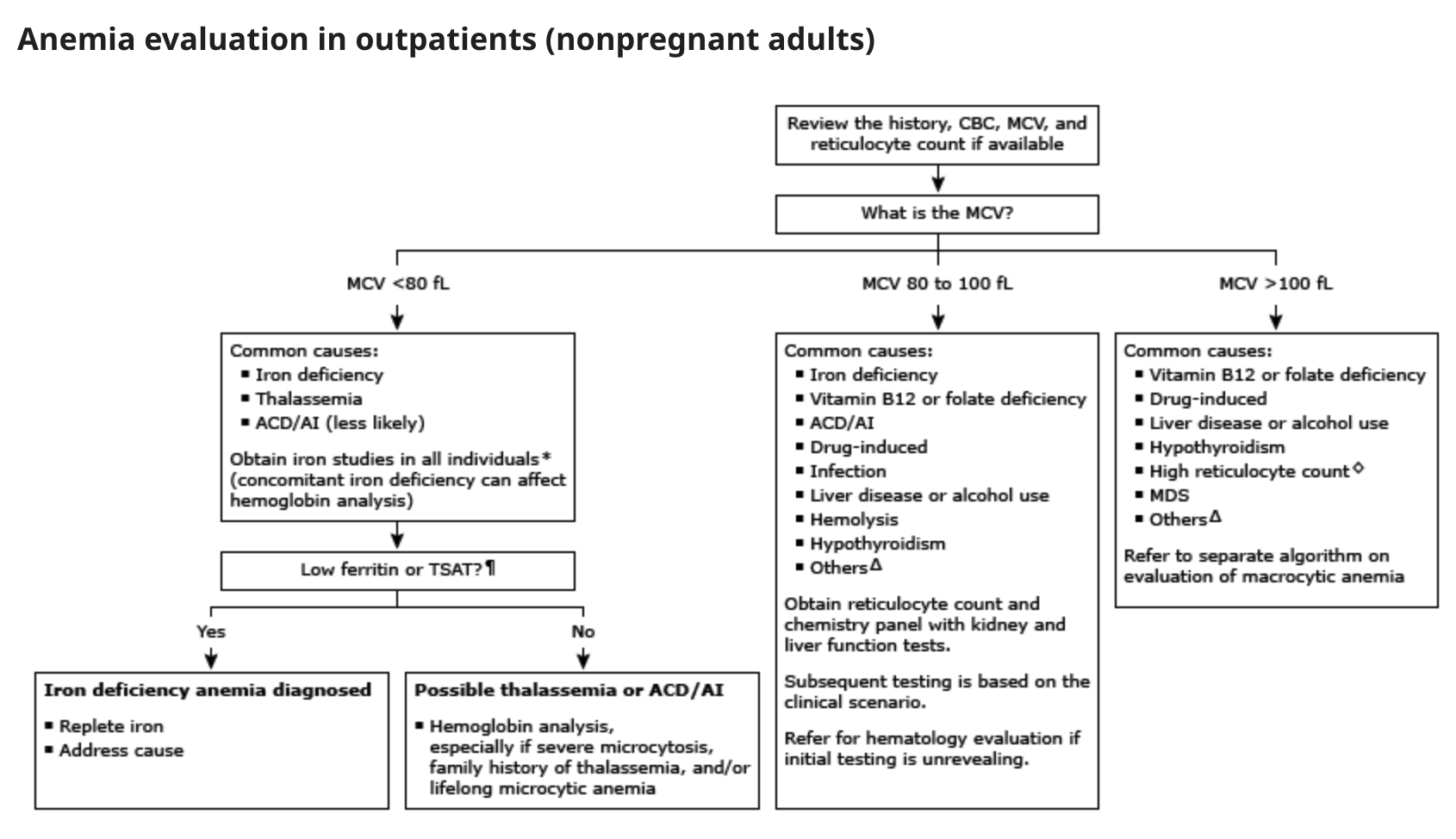

This table from UTD summarizes on the different causes of anemia depending on the MCV.
Increased reticulocyte count (increased red cell breakdown) will also require peripheral smear to narrow differential.
- Acute blood loss
- Hemolysis - including antibody mediated, cellular toxins (malaria, clostridium), trauma (valve), or hypersplenism.
- Intrinsic Defect- including enzyme deficiency such as G6PHD, SCD, or thalassemia
- Membrane Defect- including spur cell, hereditary spherocytosis or PNH
Anemia with decreased reticulocyte count
- Deficiency of Iron, Vit B12, Folate, or copper
- Medication that can suppress the bone marrow (such as quinidine, TMP SMX, albendazole)
- Primary bone marrow disorders (MDS, Myelofibrosis, or leukemia)
- Very recent bleeding (within 5-7 days, before bone marrow compensation has occurred)
If patient has Hgb of <7 in Non cardiac patient or <8 in cardiac patient we should consider blood transfusion (pRBC). (Let the patient know of the risk's and benefits and also inquire that patient is not a Jehovah's Witness before proceeding with blood transfusion).
Sickle Cell Pain Crisis
- Sickled cells occlude arterioles and cause tissue infarction, resulting in recurrent painful episodes, and a variety of serious organ system complications that can lead to life-long disabilities and even death.
- Causes: Precipitated by infection, fever, dehydration, or exposure to low oxygen tension (high altitude travel).
- Clinical manifestations: Characterized by severe pain, typically of the back, limbs, ribs, lasting 5-7 days. Pattern of pain in a given patient usually consistent from crisis to crisis. If new pain, consider an alternative diagnosis.
Treatment:
- Oral hydration with 3-4 liters of fluid per day. We sugest to start 0.5 to 1 L NS bolus, then maintainance D51/2NS at 150-250 cc/hr.
- Pain management: These patients are usually on chronic opioids. Start dose of IV morphine based on patient's prior dose requirements, or start with 2-5 mg morphine every 3-4 hours. Convert to PO once IV dose approaches equal analgesic home regimen. Perform assessments every 20 min and escalate as needed.
- Supplemental O2 if hypoxia is present. Provide incentive spirometry.
- Provide stimulant (not osmotic) laxatives.
- Avoidance meperidine (can precipitate seizures), and ketorolac (associated with AKI).
- Evaluate for SCD complications associated with pain (eg, avascular necrosis of the hip, acute chest pain syndrome, splenic sequestration). CBC, retic count, cultures, lytes, BUN, vreatinine, bilirubin, UA, CXR,blood type and screen.
Blood Component Therapy
Packed red blood cells (PRBC):
WBCs are the chief cause of alloimmunization to HLA antigens, which leads to future febrile transfusion reactions and platelet refractoriness. Indicated for patients who require long term transfusion support (Bone marrow transplant, leukemia, chemotherapy), and are at risk of becoming refractory to platelets, or with recurrent febrile reactions.
Products are irradiated to kill donor stem cells which (rarely) cause transfusion-associated GVHD.
Indicated for BMT recipients, immunosuppressed patients, when donor and recipient are blood relatives, and patients receiving HLA matched platelets.
RBC washed to remove plasma proteins, electrolytes, and antibodies. Indicated only in patients with history of severe transfusion reactions, hyperkalemia, paroxysmal nocturnal hemoglobinuria. Very expensive!
Active bleeding and one of the following:
1 - Blood loss > 500cc or 15% of blood volume (70 cc/kg body weight)
2- SBP < 100 mmHg or 20% fall in SBP
3- Pulse > 100 bpm
4- General anesthesia and Hgb < 9 g/dl
5- Chronic, symptomatic anemia (generally Hgb < 9g/dl)
6- Chronic transfusions to suppress endogenous Hgb in selected patients with sickle cell disease
7- Hgb < 10 g/dl in patients with known coronary artery disease, unstable angina, or acute MI. No RTC trial data to support this practice. One RCT (n=428) in patients undergoing CABG randomized patients to transfusion only if Hgb < 8 g/dL or standard practice (generally Hgb > 9.0) and found no mortality differences.
9- ICU mortality data with clear evidence for more restrictive transfusion (Hgb<7.0) practices
Patients with chronic anemia increase plasma volume in order to maintain an adequate cardiac output.
The volume associated with transfusion will cause overload and must be done slowly to avoid precipitating CHF (4 hours per unit vs. 5-10 min/unit in a hypotensive patient with acute blood loss).
Consider transfusing in splits of ½ volume over same time (4 hours per split is the slowest rate at which blood may be transfused).
Consider Lasix 20-40 mg IV to avoid fluid overload during transfusion of multiple units.
Platelets:
1- 1 unit single donor platelets (SDP) = 7 units of random donor platelets (a hemostatic dose for bleeding in an adult patient)
2- General dose is 1 unit random donor platelets per 10 kg body weight ≈ 1 unit single donor platelets for a 70 kg person.
3- For every 1 unit of SDP, the patient receives hemostatic levels of coagulation factors equivalent to 1 unit of fresh frozen plasma.
1- Platelet count < 5-10K in ITP or significant purpura
2- Platelet count < 10K in J patients, or patients not predisposed to spontaneous bleeding. No change in bleeding events in RCT when compared to < 20K as transfusion threshold
4- Platelet count < 20K and a clinical factor that would be associated with risk of spontaneous bleeding (Temperature > 38.5°C/Infection, concurrent coagulopathy, DIC, hepatic or renal failure, marked splenomegaly)
5- Platelet count < 50K and surgery or post-op bleeding
6- Platelet count < 50K and invasive procedure (LP, indwelling lines, liver or transbronchial biopsy, epidural puncture)
7- Platelet count < 100K with active bleeding
1- Causes: fever, sepsis, splenomegaly, DIC, drugs, platelet consumption, s/p BMT (likely multifactorial etiology, in one series < 40% post-BMT transfusions resulted in appropriate rise in platelet count), alloimmunization with antibody mediated destruction of circulating platelets (towards HLA class I antigen)
2- Diagnosis: check rise 60 minutes after transfusion.
3- Appropriate rise with decrease over next 24 hours®sepsis, DIC, post BMT, etc. No rise at 60 minutes indicates alloimmunization. Order platelet antibody screening test (results in 2-3 days).
4- Treatment: if test positive, or while results pending, order "HLA matched" platelets and check platelet count 10 minutes to 1 hour following transfusion to document appropriate rise. Minimal options in acute bleed situation.
Effort should be made to avoid alloimmunization in at risk patients through irradiation, leukocyte reduction (comparable in RCT) or both.
Fresh frozen plasma (FFP):
FFP is made by separating plasma from a unit of whole blood. Contains all clotting factors. One unit of FFP contains: 200-250 cc volume, 400 mg fibrinogen, 200 units of other factors (factors V, VII, XI, ATIII, Protein C, Protein S)
1- Active bleeding or risk of bleeding if PT and/or PTT> 1.5-1.8x normal.
2- Patient with massive bleeding at high risk for clotting factor deficiency while coags pending. Common causes of factor deficiency: liver disease, vitamin K deficiency, DIC, hemorrhage, TTP (treatment with plasma exchange)
3- Reversal of warfarin therapy. Minimal evidence that FFP can correct mildly elevated INR (< 1.8).
1- Starting dose 15 cc/kg = 4-6 units (dose needed to replace 25% clotting factors, minimum amount necessary to obtain hemostasis)
2- Maximum effect declines after 2-4 hours, so infuse rapidly at time of bleeding or no more than 1 hour prior to anticipated bleeding.
3- Administer fewer units of FFP when transfusing platelets since 1 unit SDP contains equivalent clotting factors to 1 unit FFP.
4- Consider Lasix IV when multiple units FFP given rapidly to avoid fluid overload.
Cryoprecipitate: (Contains fibrinogen, factor VIII, and von Willebrand factor)
1- Fibrinogen < 100 mg/dl (as in DIC)
2- Preparation of topical fibrin glue for surgical hemostasis
Concentrated factor VIII and von Willebrand factor are preferred treatments of Hemophilia A and von Willebrand's disease since cryoprecipitate not virus inactivated, thus carrying a higher risk for virus transmission.
1- Usual starting dose is 10 units. Each unit raises fibrinogen by about 8 mg/dl. Follow fibrinogen levels every 6-8 hours to guide frequency and quantity of administration.
Transfusion Reactions
For all reactions (except mild allergic/uricaria): STOP transfusion, send remaining blood product and fresh blood sample to blood bank)
Acute Hemolysis (caused by ABO incompatibility)
1- Stop transfusion immediately if reaction suspected!
2- Maintain blood pressure and urine output with vigorous NS hydration via new infusion set.
3- Lasix 80-100 mg, or mannitol IV to maintain urine output with goal >100 cc urine/hr.
4- Follow strict I/Os.
5- Close monitoring for any electrolyte abnormalities (hyperkalemia)
Anaphylaxis
Acute Lung Injury
Delayed Hemolysis
Bacterial Contamination
Febrile, Non-Hemolytic Transfusion Reaction
Urticaria
Infectious Disease
Antibiotic Recommendations/Dosing
General Principles
- Initiate empiric therapy based on severity of illness, likely pathogen, likelihood of drug resistance, host factors (allergy, poor renal function, immunocompromised)
- Initiate antibiotic therapy as soon as possible
- tailor antibiotic therapy based on culture results
- tailor antibiotic therapy once culture results are available (often 48-72 hours)
- Transition from IV to oral antibiotic as soon as feasible to decrease cost and reduce complications from IV access
- Consult ID for further assistance
Disease // Treatment with Dosing
Another useful app that you can access in phone (require fee) : Sanford Guide
*All drug dosing is based on immunocompetent patients with no renal or hepatic dysfunction and normal weight, not elderly and not in ICU
BONE/JOINT
Joint infections with hardware
- Consult ID and wait for results
Non-Vertebral Osteomyelitis
- Vancomycin 1000 mg IV q8h
Septic Arthritis
- Vancomycin 1000 mg IV q8h + Ceftriaxone 2 g IV q24h
CNS
Brain Abscess
- Ceftriaxone 2 g IV q12h+ Metronidazole 500 mg IV/PO q8h+/- Vancomycin 1000 mg IV q8h
Epidural Abscess
- Ceftriaxone + Vancomycin 1000 mg q8h
Meningitis (community-onset)
- Ceftriaxone 2 g IV q12h + Vancomycin 1000 mg IV q8h +/- Ampicillin 2 g IV q4h
INTRAABDOMINAL INFECTION
C. difficile (non-complicated)
- Vancomycin 125 mg PO q6h
Community-Acquired Secondary Peritonitis
- Ceftriaxone 1g IV q24h + Metronidazole 500 mg IV/PO q8h OR Ertapenem 1g IV q24h
Diverticulitis
- Ceftriaxone 1 g IV 24h + Metronidazole 500 mg IV/PO q8h
Liver Abscess
- Ceftriaxone 1 g IV 24h + Metronidazole 500 mg + Vancomycin 1000 mg IV q8h
Spontaneous Bacterial Peritonitis
- Ceftriaxone 1 g IV q24h
Traveler's Diarrhea
- if mild, fluid and electrolyte repletion +/- bismuth subsalicylate.
- If worse, Azithromycin 500 mg PO daily OR Ciprofloxacin 500 mg PO BID
PNEUMONIA
Pneumonia, Community Acquired
- Ceftriaxone 1g IV q24h + Doxycycline 100 mg IV/PO q12h
Pneumonia, Healthcare Associated
- Vancomycin 1000 mg IV q8h + Ertapenem i g IV q24h OR Cefepime 2 g IV q24h OR Piperacillin/Tazobactam 4.5 g IV q8h *Piperacillin/Tazobactam requires loading dose and infusions over 4 hours
RESPIRATORY, HEAD AND NECK INFECTIONS
Bacterial Exacerbation of COPD
- Doxycycline 100 mg IV/PO q12h OR Azithromycin 500 mg IV/PO x1 + 250 mg IV/PO q24h
Acute Sinusitis // Watchful waiting first,
- Amoxicillin 500 mg PO q8h if worsening
Peritonsillar Abscess
- Ampicillin/Sulbactam 3 g IV q6h +/- Vancomycin 1000 mg IV q8h
Pharyngitis
- Penicillin VK 500 mg PO BID
SEPSIS
Community Acquired Sepsis
- Vancomycin 1000 mg IV q8h + Ceftriaxone 2 g q24h OR Piperacillin/Tazobactam 4.5 g IV q8h OR Ertapenem 1g IV q24h *Piperacillin/Tazobactam requires loading dose and infusions over 4 hours
Fever in person who injects drugs
- Vancomycin 1000 mg IV q8h
Healthcare Acquired Sepsis
- Vancomycin 1000 mg IV q8h + Piperacillin/Tazobactam 4.5 g IV q8h OR Cefepime 2 g IV q12h OR Meropenem 1 g IV q8h WITH/WITHOUT Tobramycin 7 mg/kg IV q24h *Piperacillin/Tazobactam requires loading dose and infusions over 4 hours
SEXUALLY TRANSMITTED INFECTIONS
Gonorrhea
- If <150 kg, Ceftriaxone 500 mg IM. If ≥150 kg, Ceftriaxone 1000 mg IM
Chlamydia
- Doxycycline 100 mg PO BID
URINARY TRACT INFECTIONS
Uncomplicated Cystitis
- TMP-SMX 1 g DS PO BID x 3 days OR Nitrofurantoin 100 mg PO BID x 5 days
Acute Prostatitis
- Ciprofloxacin 500 mg PO BID OR TMP/SMX 1 g DS PO BID
Community-Acquired Pyelonephritis/Complicated UTI
- Ceftriaxone 1 g q24h
Reference:
Guidelines for Empiric Therapy: Adults | Infectious Diseases Management Program at UCSF
Adult Outpatient Treatment Recommendations | Antibiotic Use | CDC
Antimicrobial stewardship in hospital settings - UpToDate
Neurology
Seizures
Objective
The primary objectives of the medical evaluation of the first seizure are to establish whether the event was a seizure, and if so, whether it resulted from a correctable systemic process or whether the patient is at risk for developing further unprovoked seizures
Seizures are further categorized as either focal or generalized according to whether the onset of electrical activity involves a focal region of the brain or the entire cortex simultaneously. The clinical manifestations of seizures vary based on the location of the seizure in the brain and the amount of cortex that is involved.
Cause
- genetic
- structural
- metabolic
- immune
- infectious
- unknown.
Differential Diagnosis
- syncope
- transient ischemic attack
- migraine
- psychogenic nonepileptic seizures.
Work-Up
- laboratory studies (electrolytes, glucose, calcium, magnesium, complete blood count, renal function tests, liver function tests, urinalysis, and toxicology screens),
- ECG
- EEG
- neuroimaging study
- Depending on the clinical situation, a lumbar puncture may also be indicated
Management
Antiseizure medications are not always indicated after a first seizure.
In criticaly ill patients, commonly used drugs in this setting include levetiracetam, fosphenytoin/phenytoin, and valproic acid
Hospitalization may be required for patients who have a first seizure associated with a prolonged postictal state or incomplete recovery. Other indications for hospitalization include status epilepticus, the presence of a systemic or neurologic illness or injury requiring additional evaluation and treatment, and questions regarding compliance
Seizure Disorders - American Family Physician (aafp.org)
Evaluation of First Nonfebrile Seizures - American Family Physician (aafp.org)
Evaluation and management of the first seizure in adults - UpToDate
AMS
Causes
CNS insults, Systemic Infections, Metabolic Disturbances, Toxin Exposure, Medications, Chronic Systemic Diseases, Psychiatric conditions
Definition
Change in consciousness, appearance, behavior, mood, affect, motor activity or cognitive function
Best Practice
Do not assume a diagnosis of dementia in elderly patients with AMS without assessing for delirium
Do not use physical or chemical restraints, outside of emergency situations. Assess for unmet needs or environmental triggers
Evaluation:
As the differential is broad, history and physical exam is always the first step to determine diagnostic testing.
- Evaluate ABC's
- Vitals, glucose, H&P
- Diagnostic studies as indicated by H&P
- Neuroimaging
- MRI brain or EEG or LP
- If still unclear, specialty consultation
Treatment
Definitive treatment is removal of the underlying cause
However, if patients' behaviors threaten self or others, then attempt nonpharmacologic interventions are the treatment of choice. This includes reassurance, family, friends and environmental factors.
Medications are used only when nonpharmacologic treatments are ineffective and only when it is essential to control behavior. These include antipsychotics, benzodiazepines and ketamine, but they contraindications and FDA warnings.
Recent-Onset Altered Mental Status: Evaluation and Management - American Family Physician (aafp.org)
Pulmonary
CAP
Common causes
Streptococcus pneumoniae (pneumococcus) and respiratory viruses are the most frequently detected pathogens in patients with CAP
Typical bacteria
- S. pneumoniae (most common bacterial cause)
- Haemophilus influenzae
- Moraxella catarrhalis
- Staphylococcus aureus
- Group A streptococci
- Aerobic gram-negative bacteria (eg, Enterobacteriaceae such as Klebsiella spp or Escherichia coli)
- Microaerophilic bacteria and anaerobes (associated with aspiration)
Atypical bacteria ("atypical" refers to the intrinsic resistance of these organisms to beta-lactams and their inability to be visualized on Gram stain or cultured using traditional techniques)
- Legionella spp
- Mycoplasma pneumoniae
- Chlamydia pneumoniae
- Chlamydia psittaci
- Coxiella burnetii
- Respiratory viruses
- Influenza A and B viruses
- Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2)
- Other coronaviruses (eg, Middle East respiratory syndrome CoV, severe acute respiratory syndrome CoV, CoV-229E, CoV-NL63, CoV-OC43, CoV-HKU1)
- Rhinoviruses
- Parainfluenza viruses
- Adenoviruses
- Respiratory syncytial virus
- Human metapneumovirus
- Human bocaviruses
Making the diagnosis
- The diagnosis of CAP generally requires the demonstration of an infiltrate on chest imaging in a patient with a clinically compatible syndrome (eg, fever, dyspnea, cough, and sputum production)
- For most patients with suspected CAP, obtain PA and lateral chest radiographs. Radiographic findings consistent with the diagnosis of CAP include lobar consolidations, interstitial infiltrates, and/or cavitations.
- For selected patients in whom CAP is suspected based on clinical features despite a negative chest radiograph, obtain chest CT.
For most patients with moderate CAP admitted to the general medical ward, obtain the following:
- Blood cultures
- Sputum Gram stain and culture
- Urinary antigen testing for S. pneumoniae
- Testing for Legionella spp (polymerase chain reaction [PCR] when available, urinary antigen test as an alternate)
- SARS-CoV-2 testing
DIFFERENTIAL DIAGNOSIS
Noninfectious illnesses that mimic CAP or co-occur with CAP and present with pulmonary infiltrate and cough include:
- Congestive heart failure with pulmonary edema
- Pulmonary embolism
- Pulmonary hemorrhage
- Atelectasis
- Aspiration or chemical pneumonitis
- Drug reactions
- Lung cancer
- Collagen vascular diseases
- Vasculitis
- Acute exacerbation of bronchiectasis
- Interstitial lung diseases (eg, sarcoidosis, asbestosis, hypersensitivity pneumonitis, cryptogenic organizing pneumonia)
Inpatient antibiotic therapy
Without suspicion for MRSA or Pseudomonas
●Combination therapy with ceftriaxone (1 to 2 g IV daily), cefotaxime (1 to 2 g IV every 8 hours), ceftaroline (600 mg IV every 12 hours), ertapenem (1 g IV daily), or ampicillin-sulbactam (3 g IV every 6 hours) plus a macrolide (azithromycin [500 mg IV or orally daily] or clarithromycin [500 mg twice daily] or clarithromycin XL [two 500 mg tablets once daily]). Doxycycline (100 mg orally or IV twice daily) may be used as an alternative to a macrolide.
●Monotherapy with a respiratory fluoroquinolone (levofloxacin [750 mg IV or orally daily] or moxifloxacin [400 mg IV or orally daily] or gemifloxacin [320 mg orally daily]) is an appropriate alternative for patients who cannot receive a beta-lactam plus a macrolide.
With suspicion for Pseudomonas
Acceptable regimens include combination therapy with an antipseudomonal/antipneumococcal beta-lactam antibiotic and an antipseudomonal fluoroquinolone, such as the following regimens:
●Piperacillin-tazobactam (4.5 g every 6 hours) or Imipenem (500 mg every 6 hours) or Meropenem (1 g every 8 hours) or Cefepime (2 g every 8 hours) or ●Ceftazidime (2 g every 8 hours; activity against pneumococcus more limited than agents listed above)
PLUS ●Ciprofloxacin (400 mg every 8 hours) or ●Levofloxacin (750 mg daily)
With suspicion for MRSA
- Empiric therapy for CA-MRSA: gram-positive cocci in clusters seen on sputum Gram stain, known colonization with MRSA, risk factors for colonization with MRSA (eg, end-stage kidney disease, contact sport participants, people who inject drugs, those living in crowded conditions, men who have sex with men, prisoners), recent influenza-like illness, antimicrobial therapy (particularly with a fluoroquinolone) in the prior three months, necrotizing or cavitary pneumonia, or presence of empyema.
- For treatment of MRSA, empiric regimens should include either vancomycin or linezolid (600 mg IV every 12 hours).
- In all patients treated empirically for MRSA, obtain a rapid nasal PCR for MRSA (when available) in addition to Gram stain and culture of sputum or other respiratory tract infection to help guide subsequent therapy.
Influenza therapy
Antibiotic Therapy for Adults Hospitalized With Community-Acquired PneumoniaThe Clinical Utility of Methicillin-Resistant Staphylococcus aureus (MRSA) Nasal Screening to Rule Out MRSA Pneumonia
Asthma/COPD Flare
Initial pharmacologic therapy
Beta adrenergic agonists
- Dose and administration – Albuterol 2.5 mg (diluted to a total of 3 mL with sterile normal saline) by nebulizer or one to two inhalations (most commonly two, occasionally four; 90 mcg per inhalation) by MDI with a spacer every one hour for two to three doses and then every two to four hours as needed, guided by the response to therapy. - Levalbuterol 1.25 mg (diluted to a total of 3 mL with sterile saline) by nebulizer at the same frequency as albuterol.
- Levalbuterol (45 mcg/actuation) by MDI is given one to two inhalations (most commonly two, occasionally four) every one hour for two to three doses, then every two to four hours as needed. When combined with ipratropium, albuterol 2.5 mg is mixed with ipratropium bromide 0.5 mg in 3 mL. Muscarinic antagonists — Suggest use of the combination of a SAMA (eg, ipratropium) and SABA for exacerbations.
- Dose and administration – When combined with albuterol for nebulization, ipratropium 0.5 mg (500 mcg) is mixed with albuterol 2.5 mg in 3 mL and given every hour for two or three doses and then every two to four hours as needed. - Combination ipratropium-albuterol soft mist inhaler (SMI) can be used, 1 inhalation, approximately every hour for two to three doses and then every two to four hours as needed, guided by the response to therapy.
Ipratropium
also available in an MDI that can be used with a spacer, 2 to 4 inhalations every hour for two to three doses, and then every two to four hours as needed.
Systemic glucocorticoids
- IV glucocorticoids administered to with a severe exacerbation, not responded to oral glucocorticoids at home, unable to take oral medication
- Dose prednisone 40 mg once daily for the majority of COPD exacerbations. Regimens range from prednisone 30 to 60 mg, once daily, to methylprednisolone 60 to 125 mg, two to four times daily.
- Duration – Range of 5 to 14 days
Antimicrobial therapy
Recommend antibiotics with at least two of these three symptoms – increased dyspnea, increased sputum volume, or increased sputum purulence.
Oxygen therapy
Supplemental oxygen be titrated to a target of 88 to 92 percent pulse oxygen saturation, rather than using high-flow, nontitrated oxygen
https://www.uptodate.com/contents/copd-exacerbations-management/abstract/1,17,
https://www.uptodate.com/contents/copd-exacerbations-management/abstract/33
https://www.uptodate.com/contents/copd-exacerbations-management/abstract/12,34,35
ttps://www.uptodate.com/contents/copd-exacerbations-management/abstract/1,12,39-41
Oxygen Therapy
●Venturi masks permit a precise upper limit for the FiO2, preferable for patients at risk of hypercapnia. Venturi masks can deliver an FiO2 of 24, 28, 31, 35, 40, or 60%.
●Nasal cannula can provide flow rates up to 6 L per minute with an associated FiO2 of approximately 40%
●When a higher FiO2 is needed, simple facemasks can provide an FiO2 up to 55% using flow rates of 6 to 10 L.
●Non-rebreathing masks with a reservoir, one-way valves, and a tight face seal can deliver an inspired oxygen concentration up to 90%
●High-flow nasal cannula (HFNC) provide supplemental oxygen (adjustable FiO2) at a high flow rate (up to 60 L/min that results in a low level of continuous positive airway pressure).
ARDS/Mechanical Ventilation
Pathophysiology:
Scattered, nonhomogeneous alveolar damage that leads to oxygenation (V/Q mismatch) problems
Diagnosis:
- Onset: within one week of a known clinical insult, or new or worsening respiratory symptoms
- Imaging: bilateral infiltrates on CXR not fully explained by effusions, nodules, or lung collapse
- Origin: respiratory failure not fully explained by cardiac failure or fluid overload. An objective assessment (eg ECHO) is required to exclude pulmonary edema if no ARDS risk factors are present
- Oxygenation: (on ventilator settings that include PEEP or CPAP >5cm H2O)
- Mild ARDS: PaO2/FiO2 ratio 200-300 mmHg
- Moderate ARDS: PaO2/FiO2 ratio 100-200 mmHg
- Severe ARDS: PaO2/FiO2 ratio <100 mmHg
Etiology:
- Direct lung injury: Pneumonia, aspiration, pulmonary contusion, fat emboli, near-drowning, inhalational injury, post lung transplantation, or hematopoietic stem cell transplant
- Indirect lung injury: Sepsis, severe trauma, shock, drug overdose, DIC, pancreatitis, cardiopulmonary bypass, transfusion of blood products (TRALI)
Management:
- Mechanical ventilation:
- Goal: Maintain adequate gas exchange until the inflammation and edema subside and minimize ventilator-induced lung injury
- ARDSnet protocol (ARMA Trial): low tidal volume (4-6 ml/kg) and low airway pressure (Pplat <30 mmHg)
- Additional therapeutic considerations
- "Conservative" fluid management: FACTT trial showed that it improves oxygenation and shortens the duration of mechanical ventilation and intensive care but does not improve 60 day mortality. Goal CVP <4, PCWP <8. Excluded patients with hypotension, pressures, HD, oliguric renal failure.
- Early neuromuscular blockade in severe ARDS: ACURASYS trial (single randomized trial) showed the use of cisatracurium in patients with severe ARDS resulted in a reduction in 90 day mortality and an increase in ventilator free days. ROSE trial did not reproduce this mortality benefit.
- Prone positioning PROSEVA randomized trial showed a reduction in mortality in patients with severe ARDS; recommended for patients with P/F < 100, consider if P/F < 150
- ECMO and high frequency oscillatory ventilation: further studies are required to evaluate high frequency oscillatory ventilation and extra-corporeal membrane oxygenation. There are no consensus guidelines but consider in P/F <80.
- Steroids should NOT be initiated in late ARDS (14 days or longer). The impact of earlier steroid therapy on mortality is uncertain, as the DEXA-ARDS trial showed reduced mortality and improved liberation from the vent but previous studies were less clear.
- Recombinant surfactant does not improve survival or ventilator free days
- Low-dose nitric oxide temporarily improves oxygenation but not mortality
- Overall care
- Identify and treat underlying causes
- Ensure adequate nutrition (preferably enteral)
- Provide GI and DVT prophylaxis
- Prevent and treat nosocomial infections early
Indications for intubation
- Is there failure of airway maintenance or protection?
- Upper airway obstruction, airway protection
- Is there a failure of oxygenation or ventilation?
- Uncorrectable hypoxemia (pO2 <70 mmHg on 100% O2 NRB)
- Hypercapnea (pCO2 >55 mmHg) with acidosis [clinical judgement for pCO2 in COPD]
- Ineffective respiration (max inspiratory force <25 cm H2O)
- Does the anticipated clinical course require intubation?
- Fatigue (RR>35 with increasing pCO2)
Initial ventilator settings
- ARDS
- Initial TV 6ml/kg PBW (range 4-8 ml/kg)
- Ventilator rate 14-22 breaths per minute
- Initial PEEP of 5 cm H2O, up to 24 cm H2O
- Non-ARDS
- Initial TV between 6-8 ml/kg PBW reasonable,
- Ventilator rate 12-16 breaths per minute
- PEEP between 3-5 cm H2O
Ware LB, Matthay MA. The acute respiratory distress syndrome. N Engl J Med 2000; 342:1334-49.
https://www.uptodate.com/contents/acute-respiratory-distress-syndrome-clinical-features-diagnosis-and-complications-in-adults
https://www.uptodate.com/contents/ventilator-management-strategies-for-adults-with-acute-respiratory-distress-syndrome
Stepwise approach to managing Asthma
Intermittent (Step 1) —
Symptoms — <2 days a week, <2x nighttime awakenings/month, SABA use <2 days/week
Preferred: SABA prn
Mild persistent (Step 2) —
Symptoms — >2 days a week, 3-4x nighttime awakenings/month, SABA use >2 days/week
Preferred: Low dose ICS
Alternative: Cromolyn, LRTA, Nedocromil, Theophylline
Moderate persistent (Step 3) —
Symptoms — Daily, >1x nighttime awakenings/week, SABA use daily
Preferred: Low dose ICS + LABA OR Medium dose ICS
Alternative: Low-dose ICS + either LTRA, Theophylline, or Zileuton
Severe persistent (Step 4) —
Symptoms — Throughout the day, Often 7x nighttime awakenings/week, SABA use several times daily
Preferred: Medium dose ICS + LABA
Alternative: Medium dose ICS + either LTRA, Theophylline, or Zileuton
Severe Persistent (Step 5) —
Preferred: High-dose ICS + LABA AND Consider Omalizumab for patients who have allergies
Severe Persistent (Step 6) —
Preferred: High-dose ICS + LABA + oral corticosteroid AND Consider Omalizumab for patients who have allergies
https://getasthmahelp.org/documents/GIST-Stepwise-Approach.pdf
Nephrology
Acute Renal Failure
What is AKI?
According to The Kidney Disease: Improving Global Outcomes (KDIGO), which it the most current and preferred definition, it is:
an increase in serum creatinine of ≥0.3 mg/dL within 48 hours OR an increase in serum creatinine of ≥50% within 7 days OR Urine output of <0.5 mL/kg/hour for >6 hours
Etiology:
1)Prerenal: Decreased renal perfusion (70% of causes)
a. Intravascular volume depletion: Dehydration, third-spacing
b. Decreased arterial pressure: CHF, sepsis,
c. Extracellular fluid loss : Burns, diarrhea, vomiting, diuretics or hemorrhage
d. Decreased CO: CHF, shock
e. Medication changes to renal vasculature: ACE-i, ARBs, NSAIDs, Tacrolimus, Cyclosporine
2)Intrinsic: classified according to the site of injury
a. Vascular Injury: afferent arteriolar vasoconstriction --> decreased GFR (Ex. TTP, Vasculitis, RAS, malignant HTN)
b. Glomerulonephritis: Includes renal (PSGN, IgA, membranoproliferative GN), hematologic dz (HUS, TTP), systemic inflammation (SLE, HSP), and pulm-renal syndromes (Goodpasture, granulomatosis with polyangitis). +hematuria( RBC casts) and proteinuria.
c. Interstitial Nephritis: analogous to an allergic rxn in the kidney, may be associated with fever, arthralgia, and rash. Allergic rxns can be due to drugs (penicillin, cephalosporin, NSAIDs, Sulfas, PPIs), autoimmune disorders (ex. SLE), infections (diphtheria, GAS), or other dzs such as sarcoidosis.
d. Acute Tubular Necrosis (ATN): cell death and necrosis from renal ischemia (prolonged hypoperfusion aka prolonged prerenal state), toxins( rhabdo, uric acid crystals, radiocontrast dye, hemolysis, amioglycosides)
3)Postrenal: Renal outflow obstruction
a. Intrarenal/tubular: crystals, nephrolithiasis
b. Ureteral: bilateral nephrolithiasis, thrombosis, edema from retrograde pyelography
c. Extra-ureteral: Bladder or cervical CA
d. Bladder neck: neurogenic bladder, autonomic neuropathy
e. Urethra: BPH, prostate CA, urethral stricture
-Evaluate for volume status, skin tenting LE edema, ascites, skin rash, purpura, bladder distension, prostate enlargement etc.
-Monitor urine output, sediment, UA, electrolytes
-Calculate FENa (collect urine sample prior to IV fluid or diuretic tx). If patient is on diuretics utilize FEUrea.
-FENa: (Una/Pna)/(Ucr/Pcr), FEUrea: (Uurea/Purea)/(Ucr/Pcr)
- Renal US to r/o obstruction or assess for hydronephrosis
-Serology for complement levels and renal biopsy if etiology is unclear.

Chronic Renal Failure
Definition
GFR <60 for 3 months or more
AND/OR
presence of kidney damage (albuminuria, sediment or anatomic abnormalities or a hx of kidney transplantation).
Stages of CKD:
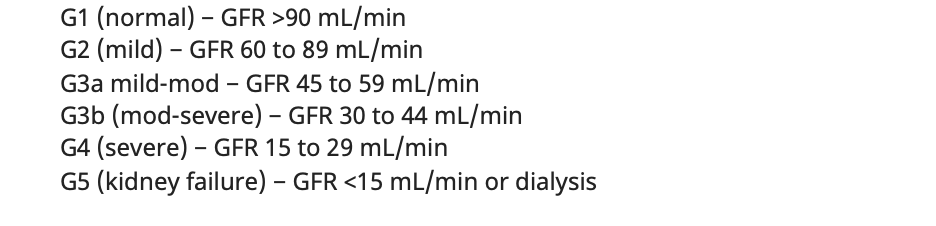
Etiology:
Most common is DM. Others are HTN/RAS, glomerular, interstitial , drugs, congenital, myeloma and PKD.
Evaluation:
-Evaluate for uremic symptoms and signs
| General | Nausea, weight loss, hypothermia |
| Skin | Pruritus, calciphylaxis(skin ulcers) |
| Metabolic |
increased K and phosphorus, decreased Ca, 2 PTH, acidosis |
| Cardio | HTN, CHF, LVH, pericarditis |
| Neuro | seizures, neuropathy. decreased memory/attention/MS (encephalopathy) |
| Heme | Anemia, bleeding(plt dysfunction) |
Management:
-Consult Nephrology if proteinuria or GRF <30. BP measurements, IVs for dialysis access planning.
-Restrict sodium, potassium, phosphorus and protein intake especially if HTN or hyperkalemic.
-Treat/ risk reduction of co-morbidities (DM, HTN, CAD) with glucose control/ SGLTi, statin, ACEi/ARB ( reassess Cr and d/c if there is a 30% increase post ACEi/ARB).
-Sevelamer to control phosphorus levels, HCO3 replete if acidotic, Fe supplementation for anemia (goal Hb 10-11.5).
-Evaluate for transplant (GFR <20)
Indications for Dialysis
Acute Indications:
Volume overload refractory to diuresis
Severe hyperkalemia (K >6.5 mEq/L) or rapidly rising K+ levels
Severe metabolic acidosis ( and pH <7.1)
Uremia (pericarditis, uremia, unexplained mental status decline)
Toxic overdose of a dialyzable drug (Barbiturates, Isoniazid, Salicylates, Methanol etc)
Chronic Indications:
CKD stage 5, GFR<15
Modalities:
Intermittent Hemodialysis (IHD): access-> AV fistula/graft
Peritoneal Dialysis (PD): access ->peritoneal catheter.
Timing:
3 times weekly, on alternate days, (MWF or TThSa) is the recommendation for intermittent hemodialysis (IHD).
Newborn Service
FM Unassigned Newborn Service
Welcome to the Family Medicine newborn inpatient service! We admit most “unassigned” babies (no pediatrician selected, or one selected that does not have permissions at St. Agnes). We are working on a list for inclusion and exclusion criteria for our service. Remember, nothing is set in stone and this will all likely change as the rotation evolves.
Written by Arianna Crediford, MD (PGY1)
-
On your first Monday morning, report to the FM rounding room at 7:00 AM to receive sign out from the night resident. Check Amion for who your attending will be and find out when they’d like to round.
-
Your best view for the list will be the LD grease board (accessed by clicking the red EPIC button in the top left corner → Patient Care → LD Grease board; can click the thumbtack on the right side to pin it). Once on the LD grease board, head to the → Nursery tab to see all the newborns, either located on 4 Main or 6 Main. You can sort by attending to see which babies are assigned to us, if any. Alternatively you can favorite the SAFR Nursery 4 Main and SAFR Nursery 6 Main lists which can be viewed on mobile unlike the greaseboard. When in baby’s chart, mom’s chart is linked at the bottom left in green and vice versa. You will need to check her chart for more in-depth OB history. The “delivery” tab (which is identical in mom and baby’s chart) has most of the other info you will need.
-
Important: Once sign out is received for the morning, go to the 6th floor main newborn nursery and introduce yourself to the nurses, leave a post-it with your name and attending’s name for the week so they know who to Haiku with the admission sheets known as “pink sheets” for new babies.
-
Nurses may call the Newborn phone (phone by printer in FM rounding room) prior to Haiku. Make sure to intermittently check the LD grease board to ensure babies are not assigned to our attending without our knowledge.
-
Weekday AM shifts we work with our FM attendings, no cross coverage. You can always contact the pediatrician on call for complicated babies/questions. (Amion- ED CALL- Unassigned Newborn)
-
Weekend AM shifts + all PM shifts we work with the pediatricians as attendings. If our service still has babies on the weekend, keep them assigned to our attending (DO NOT reassign to pediatrician to avoid confusing the services). Round with the pediatrician and discuss with them how they would like notation to be handled.
-
We don't take new admissions on weekends or nights; instead we cross cover for all pediatricians; all new babies are assigned to the pediatrician, healthy babies do not need to be seen unless concerns or calls. Contact the on-call pediatrician so they have your number and ask for any additional instructions, e.g. which babies to watch out for overnight.
- When Dr. Thampy is on she has a nurse practitioner Frances Cipolla who is not on AMION but can be reached at 559-285-3985. She has been working 25+ years and is a brilliant resource
-
Useful Tips
Admissions: .NBHPFAM (EPIC, if it doesn't auto populate, search Phillip Kim in Personalization and use the SHARE ICON for access)
-
Wait for pink sheets to be sent by nurses via haiku for new admissions. Nurses do a mini-triage to decide if the baby is healthy enough for our service; if not it will be assigned to the pediatrician.
-
Make sure to do your own triage for missed warning signs/risks; if concerns can call pediatrician and reassign baby to them or even NICU as indicated. Do not give back to nurses/reject baby.
-
-
Pink sheets sent usually about 30-45 min after birth: includes all delivery info, maternal risk factors, most highlights that you would want to know but always double check chart
-
Generally we don’t put in orders unless Bili work up, sepsis work up, or sometimes to add formula.
- May need to check mom’s chart for patient location since it is not always updated on baby’s chart; check mom’s chart for OB history as well. Ensure mom is RPR neg x 2 (one prenatal, one at delivery).
-
Try to see baby within 2 hours of being born: full physical exam, find out who pediatrician is (if none selected try to recruit to our clinic by messaging Deb mom’s MRN and she will call pt and make appt), find out feeding plan (breast vs formula vs both), and parental concerns. Baby must be seen absolutely no later than 24 hours after birth. Mom and baby will be on 6th floor at first then moved to 4th floor. May be in the recovery room (RR) which is on 6th floor especially if C-section. On 4th floor, nurse takes care of mom and baby so can answer questions about both for you.
-
Note templates: submit to FM attendings on weekdays. Find out if the pediatrician wants you to write notes on weekends. No notes or admissions at night.
-
.NBHPFAM : H&P template for new admissions
-
.NBPNFAM: Progress note template
-
.NBDCFAM : Discharge summary template
-
-
Please add additional issues to assessment and plan as appropriate e.g. maternal GBS positive or GDM, LGA/SGA, systolic murmur, sacral dimple, etc.
Cap: 12 total notes or 6 total admissions for the day. No more than 12 INTERACTIONS/NOTES per day. So if you start the day with 12 babies on the list and you discharge 6, you don't have to admit 6 more. This will likely change as the rotation evolves.
Progress Notes: .NBPNFAM
-
If baby is LGA or SGA, maternal GDM, mom got labetalol, or other glycemic risk factors nurses will put orders to monitor POC glucose automatically. If POC glucose low per UTD chart (in rounding room) can check serum glucose, consider treating per serum glucose.
-
If SGA or preterm, may need car seat challenge prior to d/c which nurses will automatically do
-
Sepsis work up: Blood cultures x 2, CBC, CRP if indicated (can use EOS to assist)
-
Screenings: At 24 hours of life three screenings are performed: hearing screening, pre and post ductal O2 sat for congenital heart defect screening, and bilirubin screening (transcutaneous Tc). If normal, most babies are clear for discharge. If Tc Bili is elevated per bilitool, can order serum bili (total and direct) since Tc Bili tends to overestimate bilirubin. If baby has jaundice risk factors (direct coombs positive, ABO incompatibility) or visible jaundice/ruddiness on exam, can do Tc bili earlier @ 6 hours or 12 hours of life.
-
Can check screenings under chart review- → single click on current encounter → flowsheets → screening
-
Alternatively, flowsheets tab can be used and newborn screening can be pinned- can discuss with Arianna or Dr. Kim to have pinned
-
Indirect coombs is done with mom’s blood and can be seen on mom’s chart or pink sheet as “Maternal Ab” status positive or negative. Baby’s blood type and direct coombs are assessed from cord blood gas, usually results back by 24 hours of life.
-
-
NICU is on 4th floor, can discuss cases with their attendings at any time.
-
Make sure red reflex is done prior to D/C- ophthalmoscope can be found at 4th or 6th floor nursing stations
Discharges: .NBDCFAM
-
NSVD births: max stay is 24 hours unless complications
-
C-Section births: max stay is 72 hours unless complications
-
Ensure red reflex is done
-
Cannot leave without pediatrician selected and documented, ensure car seat, ensure screenings are done (hearing, heart, bili as above)
-
Nurses will let you know when mom is clear for d/c and ask if baby is good to go but you can also check mom’s chart
-
Can consider adding vitamin D drops in discharge orders upon D/C (can find in Dr. Kim’s preference list)
-
Discharge summary has a hospital course template generated for ease but please read through and add additional complications/findings as appropriate; remove sentence about blood sugar checks if not performed.
Toxicology
ETOH Intoxication
Management:
- Ensure airway, adequate respiratory drive, and management of secretions/emesis
- Thiamine, consider folate/MVI, D5NS (for volume and glycogen/NAD+ depletion - will not enhance elimination )
- Check FSBG. Hypoglycemia is caused by impaired gluconeogenesis in poorly nourished patients with depleted or low glycogen stores.
- Search for other causes if mental status not clearing in 3 to 4 hours.
- Alcoholic ketoacidosis: Volume repletion, thiamine, and supplemental glucose
- Start CIWA protocol for all suspected chronic alcoholics
Symptoms:
1. Tremulousness (6-12 hours after last drink)
- Pt irritable, hypervigilant, agitated. coarse tremor of hands and tongue
- Thiamine 100mg IV, MVI, Folate 1 mg IV/PO. Give thiamine before glucose
- Mg replacement, watch for drop in phosphate
- Valium 5-10 mg IV q5-10min until stops or Librium 25-100 mg PO hourly. Monitor closely for oversedation
2. Seizures
- If no past h/o seizure, work up to r/o head trauma, meningitis, brain abscess, etc.
- If past h/o EtOH seizure, treat as other seizures but loading with anticonvulsants not indicated
3. Delirium Tremens - autonomic instability with fluctuating mental status. 2-7 days after last drink, usually with visual hallucinations, perspiration, fever, tachycardia, hypertension. This is a medical emergency. mortality is approx. 5%
- Valium 5-10 mg IV every 5 to 10 minutes until appropriate sedation is achieved.
- Librium 25-100 mg PO at presentation, repeat as needed hourly. Monitor respirations.
- Thiamine, folate, MVI iv/po
- Replete Mg, K, Ca, PO4
- Rule out infection, pneumonia
- Admit to monitored setting
Other toxic alcohols:
- Send ethanol level to calculate corrected osmole gap in the case of suspected concurrent ethylene glycol or methanol ingestion.
- Toxic alcohol panel (ethylene glycol, methanol, isopropyl alcohol) can be sent but do not delay treatment if clinical suspicion is high.
- Most common differential diagnosis is alcoholic ketoacidosis, which can cause severe anion gap acidosis and moderate osmolar gap. Send a beta hydroxybutyrate level, which is more reliable than standard ketone test (acetoacetate).
References:
Kraut JA, Kurtz I. Toxic alcohol ingestions: Clinical features, diagnosis, and management. Clin J Am Soc Nephrol 2008 Jan;3(1!):208-25.
Goldfrank's Toxicology Emergencies, 9th ed 2010.
Poisoning and Drug overdose, 6th ed. 2012.
UpToDate. (2022). https://www.uptodate.com/contents/management-of-moderate-and-severe-alcohol-withdrawal-syndromes.
Acetaminophen Overdose
Check Acetaminophen levels and urine toxicology for co-ingestions
- Call poison control
- NGT, lavage with 2 L NS
- Activated charcoal: Give a single dose of activated charcoal at 1 g/kg p.o. via NG tube within 4 hours of ingestion
- N–Acetylcysteine: Passive given within 8 hours of ingestion and before ALT begins to rise, can give a charcoal
- Oral dosing of acetylcysteine: 140 mg/kg loading dose followed by 17 doses of 70 mg.kg every 4 hours. If patient vomits within 1 hour administration give full dose again
- Give acetylcysteine based on the nomogram. If unable to obtain level just treat.
- Follow acetaminophen levels q4h, LFT, PT/PTT
- Evaluate potential need for liver transplant; pH < 7.3, Cr > 3.4, INR >6.5
References:
1. Hospitalist Handbook, iPhone App
2. UpToDate -- Acetaminophen Overdose
3. NCBI
Salicylate Overdose
Check salicylate level and check urine toxicology for co-ingestions. Try to determine whether salicylate was regular or enteric-coated (Affects pharmacokinetics).
- Call poison control
- NGT, lavage with 2L NS
- Intubate for respiratory depression if indicated
- Activated charcoal, if indicated. 1g/kg po/per NGT q2-4h
- Alkalinize plasma/urine with a bolus of 1 to 2 Amps of sodium bicarb, then start 2 Amps of sodium bicarb per 1 L of D5 ¼ NS. Run this at approximately 4 mL/kg/hr. Do not use acetazolamide. Caution in elderly and renal failure as aspirin can cause pulmonary edema
- Replete potassium to maintain normal serum levels otherwise alkalinization will be difficult to achieve
- Be sure to treat concurrent hypoglycemia and coagulopathy if present
- External cooling if febrile (no acetaminophen)
- Hemodialysis indicated if level > 100mg/dL - level checked 6 hours after ingestion, refractory acidosis, persistent CNS symptoms, and/or if renal failure.
References:
1. Hospitalist Handbook, iPhone App
2.UpToDate -- Salicylate Toxicity
TCA Overdose
Call poison control.
- Check urine toxicology for co-ingestions esp. salicylates , acetaminophen.
- Get an EKG. Pay special attention to QRS, QTc, PR Beware QRS on EKG> 0.10 sec; VT, VF, myocardial depression can ensure (Q on T phenomenon)
- Evaluate if ICU admission is necessary: AMS, Respiratory depression, hypotension
- Telemetry
- If asymptomatic, get serial EKGs for 6 hours.
- NGT, lavage with 2 Liters NS, Ipecac contraindicated
- Activated charcoal 1g/kg within 2 hours of ingestion
- Alkalinize urine with 1NS & 2amps NaHCO3/I at 10-15 cc/kg/hr until urine output good, then D5W + 1-4 amps NaHCO3/I + 200 mEq KCl/I at 1-3x maintenance to give serum pH 7.5-7.55
- Do NOT use quinidine, procainamide if VT occurs. High risk for Torsades.
References:
1. Hospitalist Handbook, iPhone App
Cocaine Overdose
- Call Poison control
- ABCs, vital signs, Tele monitor
Diagnosis
- EKG, CXR, head CT if suspect cerebral hemorrhage.
- Labs: Urine toxicology, CBC, electrolytes, glucose, CPK, UA for myoglobin, lactic acid, Troponin, Pregnancy test.
Management
- For tachyarrhythmias, follow ACLS guidelines. Do best to avoid Beta-blocker but if needed, give IV esmolol.
- For HTN, give Benzodiazepine. If this does not work then consider Beta-blocker (esmolol), but never alone. Always give with either vasodilator (nitroprusside) or alpha blocker (phentolamine, intravenous (IV) bolus. The usual dose is 5 to 10 mg IV every 5 to 15 minutes as necessary.)
- For agitation and psychosis, Benzodiazepine(Diazepam be given in an initial dose of 10 mg IV, then 5 to 10 mg IV every 3 to 5 minutes until agitation is controlled), Haldol, chlorpromazine, or droperidol prn
- For seizures give diazepam (0.1-0.2 mg/kg IV q10-15 min for total of 30mg), but if status epilepticus, consider other causes such as continued drug absorption (broken bag of cocaine in GI tract)
- Decontaminate with gastric lavage, charcoal and cathartic if indicated.
- If need to intubate, avoid succinylcholine since this can cause further rhabdomyolysis
Source: Uptodate: Cocaine Overdose
Hospitalist Handbook
Opiate Overdose
Effects
- CNS - sedation and respiratory depression, seizures w/ meperidine, propoxyphene and dextromethorphan (Esp. in renal insult)
- Pulmonary - acute noncardiogenic pulmonary edema
Diagnosis
- H&P (pinpoint pupils, CNS and resp. depression)
- Response to naloxone
- Labs: urine tox (will not show fentanyl), CBC, eletrolytes, glucose, ABG, CXR, consider acetaminophen/ASA levels if combination drugs ingested
Treatment
- ABCs, oxygen
- Naloxone 0.2-2mg IV, may repeat dose q2-3 min up to total of 10-20mg IV. Necessary to monitor at least 3-4 hours after last naloxone dose which has half-life of 1 hour. Opiates have longer half life. Recommend 6-12 hour observation after opioid-induced coma and monitor for acute withdrawal syndrome in opiate dependent patients.
- If patient is intubated for airway protection/hypercarbia, naloxone is not necessary
- Decontaminate via gastric lavage, charcoal, cathartic.
Source: Uptodate: Opiate overdose
Carbon Monoxide Inhalation
Symptoms depend on CO level (carboxyhemoglobin)
- CO: 20-40%: Dizziness, headache, weakness, disturbed judgement, decreased visual acuity
- CO: 40-60%: Tachycardia, tachypnea, ataxia, syncope, seizures
- CO: >60%: Coma, death
Diagnosis
- To get CO level, get ABG with carboxyhemoglobin
- Standard pulse oximetry (SpO2) CANNOT screen for CO exposure, as it does not differentiate carboxyhemoglobin from oxyhemoglobin
- ECG, troponin if CO intoxication confirmed.
Management
- Treat with 100% O2 by tight-fitting mask or ET tube
- Intubation can be considered in severe cases (carboxyhemoglobin > 25%)
- Hyperbaric Oxygen if CO>25%
- Measure CO level q2-4h until <10%
- Must continue treating until carboxyhemoglobin is <5%
- Call Poison control
Source: Uptodate: CO poisoning
OB/GYN
Rotation expectations
Call group (only cover patients of the following):
Dr. Vishwanath
Dr. Dickinson
Dr. Marquez
Dr. Gade
Dr. Matharu
Any unassigned patients
Door Codes:
Sleep Rm 4th floor 611#
6th floor doctors’ lounge 33115
From elevator on 6th floor 425#
From COVID area to 6th floor 425
Expectations:
Round on postpartum patients - 4th floor
Round on Antepartum patients - 6th floor
Cover patients in L&D
See all patients in OB ED - 4th floor
Assist for CSs (Surgery is on 2nd floor close to main elevator)
Read NSTs
Cover GYN consults in ER or floors
Postpartum Rounds
Post Op Fever:
Wind - atelectasis
Water - UTI
Wound - infection
Walk - DVT
Wonder drug - heparin
Woman - mastitis, breast engorgement
Womb - endometritis, pelvic vein thrombophlebitis, TOA
Postpartum Hemorrhage:
Can happen postpartum often!
Pre Delivery Hgb → Post Delivery Hgb
Significant drop is > 2
- Oxytocin 20-80 IU/500ml NS IV infused over 10 mins, then 250ml/hr
- Methergine 0.2mg IM or PO (contraindication: HTN)
- Hemabate 0.25mg IM (contraindication: asthma)
- Misoprostol 200 mcg (up to 3 tabs PR or 1 tab PO)
- TXA 1gm/100ml NS IV over 10 minutes
Post-Partum Counseling
- Breastfeeding or Bottle Feeding? - Takes 3-5 days for milk letdown; longer in c/s patients
- Contraceptive Counseling
A) COC's - wait 3 wks postpartum (early Estrogen increases risk for DVT)
- estrogen may cause decrease milk production if breastfeeding-would not start in house but should not wait for 6 week check to do so
B) Progestins- can give immediately post-partum if desired
- Depo provera 150 mg IM q3 mo-same as above
2. IUD - at other institutions is placed immediately postpartum, but more likely can be placed ANYTIME after delivery
3. MIcronor 0.35 mg pill po qd
Post partum Vaccine
- Rubella - if nonimmune or equivocal, need vaccine]
- If Rh negative - check infant
If infant positive → Rhogam
If infant negative → none
Routine Visit Schedule
The first visit of prenatal care typically occurs in the first trimester. The frequency of follow up is based on the individual needs and assessment of risks.
In General, this is what we follow:
- Risk assessment and patient education is initiated at the first prenatal visit. The discussion during first visit should include scope of care that is provided, past medical, genetic, obstetric history, medications, lab studies, expected course of pregnancy, signs and symptoms to be reported to health care team, anticipated schedule of visits, risk counseling including substance use disorder.
- After initial visit, return visit every 4 weeks for the first 28 weeks.
- After 28 weeks, return visit every 2 weeks until 36 weeks.
- After 36 weeks, return visit weekly until delivery.
- If patient is high risk or having any medical/obstetrical complication, patient may be seen sooner.
Remember to always check fetal heart tone with doppler for every pregnant visit especially >12 weeks
Remember urine dip EVERY VISIT!
Start measure the fundal height of uterus after 20 weeks (expect approx 1cm fundal height growth per week of gestation)
Guidelines to Perinatal care Chapter 6
Routine Testing Intervals/Schedules
Initial Visit or First trimester visit:
- Prenatal Panel: CBC, GC/Chlamydia, HIV, Rubella, RPR, HBsAg, UA, Urine culture, Blood type, Rh (D), Antibody
- First trimester screening between 10 weeks to 13 6/7 weeks of pregnancy
- Pap smear at 21 y.o and older, if indicated
- First trimester ultrasound
- Assess risk factors and if positive risk factors consider:
- Referral to perinatologist
- Fully integrated prenatal screening, 1hr GCT, PIH panel, TSH, TB testing, Microalbumin urine or 24hr
- Vaccine: Flu in season, IMPRESS need for COVID vaccination as early in pregancy as possible
- Counseling: Diet/Exercise/Meds/Breastfeeding (EVERY VISIT for BF'ing)
14 to 20 weeks:
- 2nd trimester screening and AFP (15 0/7-19 6/7 weeks)
- Sono: 2nd TM US (18-24) for anomalies and growth
- Vaccine: flu in season
20 to 32 weeks:
- Labs: Repeat CBC and RPR for 2nd TM
- Glucose Tolerance Test after 24 weeks
- RhoGam at 28 weeks, after repeat testing for antibodies
- Vaccines: flu in season, Tdap at 27+ weeks
- Counseling: Kick count and PTL precautions at 28 weeks onwards
32 to 36 weeks:
- Vaccines: flu in season, Tdap if not received already
- Labs: Rpt CBC, GC/chlamydia, RPR during third TM
- Sono: if needed for placental location
- Fetal position (vertex or breech)
- Hospital registration at 34+ weeks
- Fill out BTL consent in cases of desired sterilization with c-section. Send a copy to L&D
- Counseling: Epidural/Lactation/Contraceptives
36 to 40 weeks:
- Send GBS
- Start NST monitoring at 40 weeks
- Set proper expectations for induction at 38-39 weeks and consider induction at 40-41 weeks
Perinatal Care Chp 6. Page 159
Prenatal Genetic Screening Test
Pregnancy Dating
Step 1: Document First day of the last normal menstrual period then use Nigel's rule or use uptodate EDD calculator to estimate EDD
-
If pregnancy resulted from assisted reproductive technology (ART), the ART-derived gestational age should be used to assign the estimated due date (EDD). For instance, the EDD for a pregnancy that resulted from in vitro fertilization should be assigned using the age of the embryo and the date of transfer.
Step 2: Compare with EDD from first TM ultrasound. Look at Table 1 to see if we should use EDD based on LMP or US
-
Ultrasound measurement of the embryo or fetus in the first trimester (up to and including 13 6/7 weeks of gestation) is the most accurate method to establish or confirm gestational age.
Step 3: Determined EDD
- As soon as data from the last menstrual period (LMP), the first accurate ultrasound examination, or both are obtained, the gestational age and the EDD should be determined, discussed with the patient, and documented clearly in the medical record.

-
A pregnancy without an ultrasound examination that confirms or revises the EDD before 22 0/7 weeks of gestational age should be considered suboptimally dated.
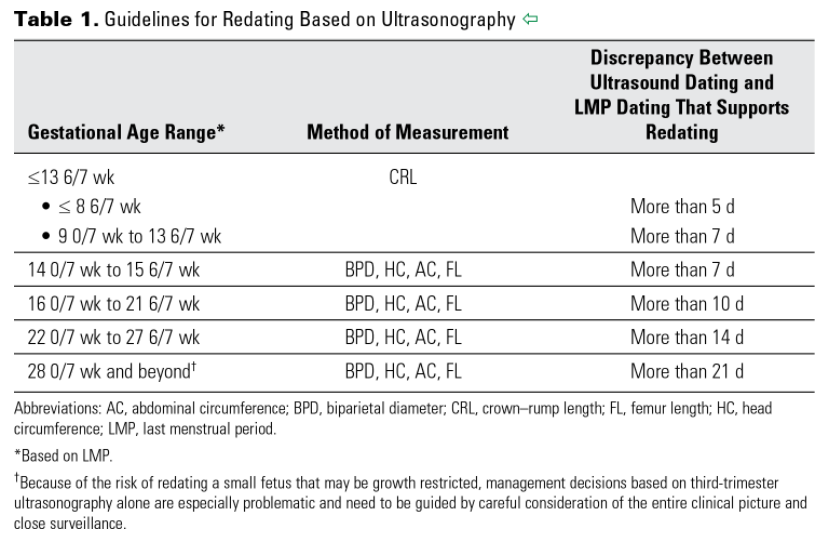
Fetal Well-Being
These are ways used to establish fetal well being:
- Fetal movement count
- Non-stress test
- Contraction stress test
- Amniotic fluid index
- BPP
- Fetal survey for anatomy and growth
- Umbilical artery doppler velocimetry
These test are used to follow:
- GDM
- IUGR
- Chronic hypertension, Pregnancy induced hypertension, preeclampsia
- Polyhydramnios or Oligohydramnios
- Multiple gestations
- >40 weeks gestation
- Any fetus at risk of hypoxia
- Change in fetal movement as perceived by the patient
- Maternal thyroid disease
- Previous stillbirth
- Fetal anomalies
ACOG Guidelines on Antepartum Fetal Surveillance
Intrauterine Growth Restriction
Definition
Sonographic EFW <10th percentile
Etiology
Maternal factor: Behavioral (smoking, substance use, decrease nutritional intake), Medical (Diabetes, HTN, renal insufficiency, autoimmune), extreme of maternal age
Fetal factor: Chromosomal or genetic cause, fetal infection, multiple gestations
Physical examination
Suspect if fundal height < dates or poor maternal weight gain
Magagement
- Growth ultrasounds every 2-3 weeks
- Antenatal testing
- twice weekly NST to once weekly BPP with NST or weekly NST with weekly AFI
- Umbilical artery doppler weekly
- Perinatology consult and consider delivery if poor NST/AFI/BPP , abdominal circ <4 wks biparietal diameter, oligo or doppler umbilical artery end diastolic flow zero or reversed
Pocket Obstetrics and gynecology by K Joeph Hurt 2nd edition
Nonstress Testing
Contraindications:
Gestational age <24 weeks
Interpretation:
>32 weeks
Reactive NST: two fetal heart rate accelerations within a 20-minute interval, peaking at least 15 beats per minute above the base line and lasting 15 seconds
<32 weeks
Reassuring for gestational age: two fetal heart rate accelerations 10 beats above the baseline and lasting for 10 seconds within a 20-minute interval.
Contraction Stress Test
The contraction stress test is interpreted by the presence or absence of late fetal heart rate decelerations.
-
Negative: No late or significant variable decelerations.
-
Positive: Late decelerations following 50 percent or more of contractions (even if the contraction frequency is fewer than three in 10 minutes).
-
Equivocal-suspicious: Intermittent late decelerations or significant variable decelerations.
-
Equivocal-hyperstimulatory: Fetal heart rate decelerations that occur in the presence of contractions that are more frequent than every two minutes or last longer than 90 seconds.
-
Unsatisfactory: Fewer than three contractions in 10 minutes or a tracing that is not interpretable.
Relative contraindications to the contraction stress test usually include conditions that are associated with an increased risk of preterm labor and delivery, uterine rupture or uterine bleeding.
Biophysical Profile
Scoring: The non stress test (2), fetal breathing movement (2), Fetal tone (2), Fetal movement (2), amiotic fluid (2)
-
Eight to ten is usually considered normal.
-
Six is considered equivocal (uncertain).
-
Four or less is considered abnormal.
- To get 2 points of breathing : one or more episodes of rhythmic fetal breathing movements of 30 seconds or more within 30 minutes)
- To get 2 points of movement: three or more discrete body or limb movements within 30 minutes
- Fetal tone: one or more episodes of extension of a fetal extremity with return to flexion, or opening or closing of a hand
- Amniotic fluid: a single vertical pocket of amniotic fluid exceeding 2 cm is considered evidence of adequate amniotic fluid
The modified BPP combines the nonstress test and an evaluation of the amount of amniotic fluid called the amniotic fluid index (AFI).
The largest pocket of amniotic fluid is measured in each of the four quadrants of the mother's abdomen using ultrasound. All four quadrants added together give the amniotic fluid index.
- AFI: < 5: oligohydramnios ; >25: polyhydramnios
Fetal Heart Rate Monitoring
BASELINE FHR
The normal FHR range is between 120 and 160 beats per minute (bpm). The baseline rate is interpreted as changed if the alteration persists for more than 15 minutes.
FHR VARIABILITY
Prematurity decreases variability therefore, there is little rate fluctuation before 28 weeks. Variability should be normal after 32 weeks.
Beat-to-beat or short-term variability is the oscillation of the FHR around the baseline in amplitude of 5 to 10 bpm.
Long-term variability is a somewhat slower oscillation in heart rate and has a frequency of 3 to 10 cycles per minute and an amplitude of 10 to 25 bpm. Clinically, loss of beat-to-beat variability is more significant than loss of long-term variability and may be ominous.
Decreased or absent variability should generally be confirmed by fetal scalp electrode monitoring when possible.
Increased variability in the baseline FHR is present when the oscillations exceed 25 bpm. This pattern is sometimes called a saltatory pattern and is usually caused by acute hypoxia or mechanical compression of the umbilical cord.
FETAL TACHYCARDIA
Baseline heart rate greater than 160 bpm and is considered a non-reassuring pattern. Mild when the heart rate is 160 to 180 bpm and severe when greater than 180 bpm.
FETAL BRADYCARDIA
Fetal bradycardia is defined as a baseline heart rate less than 110 bpm.
Bradycardia in the range of 100 to 110 bpm with normal variability is not associated with fetal acidosis. Bradycardia of this degree is common in post-date gestations and in fetuses with occiput posterior or transverse presentations.
Moderate bradycardia of 80 to 100 bpm is a nonreassuring pattern.
ACCELERATIONS
The presence of at least two accelerations, each lasting for 15 or more seconds above baseline and peaking at 15 or more bpm, in a 20-minute period is considered a reactive NST.
EARLY DECELERATIONS
Early decelerations are caused by fetal head compression during uterine contraction, resulting in vagal stimulation and slowing of the heart rate. This type of deceleration has a uniform shape, with a slow onset that coincides with the start of the contraction and a slow return to the baseline that coincides with the end of the contraction.
LATE DECELERATIONS
Late decelerations are associated with uteroplacental insufficiency and are provoked by uterine contractions. Any decrease in uterine blood flow or placental dysfunction can cause late decelerations.
A late deceleration is a symmetric fall in the fetal heart rate, beginning at or after the peak of the uterine contraction and returning to baseline only after the contraction has ended
VARIABLE DECELERATIONS
Variable decelerations are shown by an acute fall in the FHR with a rapid downslope and a variable recovery phase.
https://www.aafp.org/pubs/afp/issues/1999/0501/p2487.html
Laboratory Values in Pregnancy
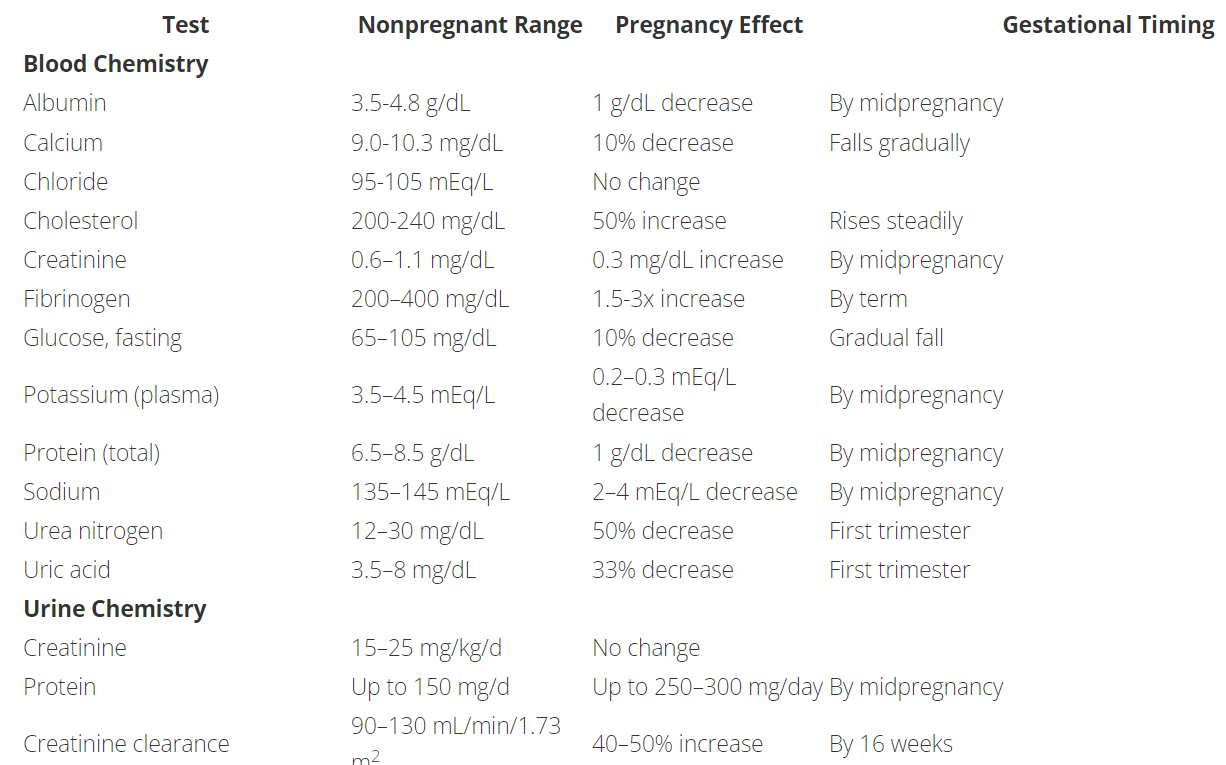
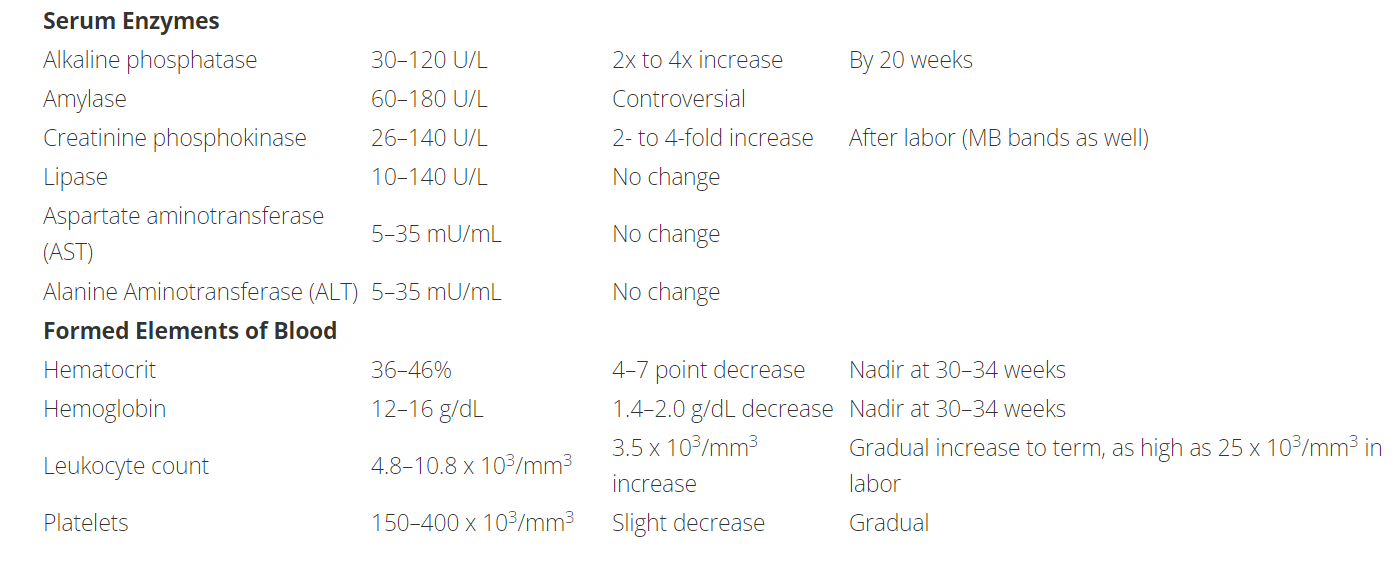
Bishop Score
The Bishop score may be used to rate the readiness of the cervix for labor.
- Scores ≤ 5 suggest an unfavorable cervix, and that induction may be necessary for successful vaginal delivery.
- Scores 6-7 do not definitively predict whether or not induction will be successful. Consider induction or augmentation of labor based on clinical judgment.
- Scores ≥ 8 suggest spontaneous vaginal delivery is more likely and augmentation or induction may be unnecessary
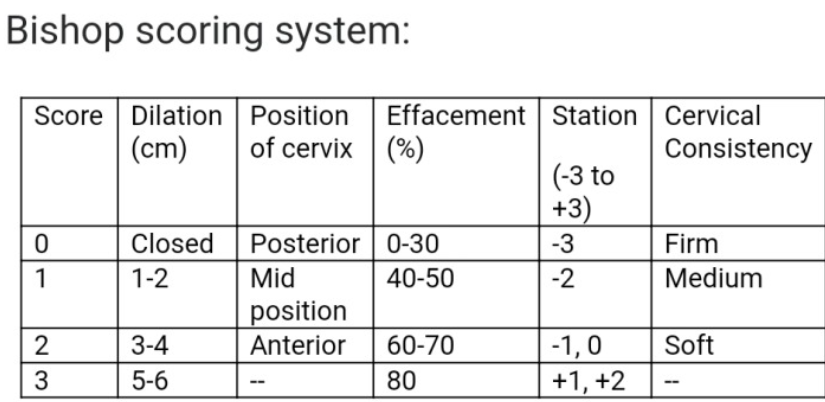
Recurrent Pregnancy Loss
Definition
3 or more consecutive preg losses before 20wk gest or after 2 consecutive losses, esp if age >35 y.o
Evaluation
- Determine actual gestational age at time of miscarriage rather than time of onset sx
- Ask about hx of thrombosis or prev fetal death, dysmenorrhea or menorrhagia ; chronic medical conditions such as thyroid dz, diabetes, or autoimmune dz such as lupus; smoking, toxins, obesity, EtOH use, excessive caffeine use
Diagnostic Workup
- Genetic (parental)
- Antiphospholipid Ab w/u: Lupus anticoagulant, beta 2 glycoprotein Ab (IgM/IgG) and anticardiolipin Ab (IgM/IgG). Need 2 positive tests 6-8weeks apart to make dx
- Consider thrombophilia w/u only if patient has a hx of thromboembolism. Test for favtor V Leiden, prothrombin G20210A mutation, protein C/S, antithrombin III deficiency
- Evaluate uterine cavity using pelvic US, hysteroscopy
- No dx is made in 50% of cases of recurrent pregnancy loss
Pocket Obstetric and Gynecology by K Joseph Hurt, 2nd edition
Hyperemesis Gravidarum
Definition
Nausea and vomiting in pregnancy that significant enough to cause dehydration, metabolic alkalosis, ketonuria, weight loss (>5%), hypokalemia
Risk Factors
Multi gestation, Family history or personal hx in prior pregnancy
Labs
CBC, lytes, UA, TSH, LFT
Therapy
IV hydration with dextrose +/- thiamine
hospitalization for monitoring
Pharmacotherapy
Diglecis
Ondansetron 4 to 8 mg q8hr
Promethazine 12.5 to 25 q4-6hr
Metoclopromide 5 to 10mg q8hr
Diet
Usually begin with a diet consisting of bananas, rice, applesauce and toast (BRAT diet) and then advance the diet as tolerated.
Hypertension in Pregnancy
Definition
Chronic HTN: SBP greater equal to 140 or DBP greater equal to 90 prior to 20 weeks or persisting longer than 12w post partum
Gestational HTN: SBP greater equal to 140 or DBP greater equal to 90 after 20 weeks with or without proteinuria
Pre-eclampsia: New onset HTN (SBP >140 or DBP >90 x2 greater than 4hrs apart) with proteinuria more than 20 weeks. Proteinuria defined as >300mg/24hr (or 1+ urine dip or urine protein:creatinine ration of >0.3). If severe features are present, proteinuria is NOT needed for the diagnosis.
Severe features: SBP >160 or DBP >110; thrombocytopenia <100,000; elevated liver enzyme test more than 2x upper limit of normal, severe RUQ pain, renal insufficiency (cr >1.1 or doubling of baseline value); pulmonary edema; new onset cerebral/visual sympmtoms
Eclampsia: Pre-eclampsia with seizures
Diagnostic work up
CBC. CMP (evaluate liver and renal function), assessment of proteinuria (by urine spot prot to creatinine ratio, UA, or 24h urine collection)
Treatment and Medication
Acute HTN
Labetalol: 20mg IV, rpt at 10 min intervals, double dose with max dose of 80mg at 1 given time; total max dose of 300mg
Hydralazine: 5-10mg IV over 1-2 min, rpt a 20 mins interval. Max dose of 30mg
Nifedipine: 10mg PO, rpt at 20 min interval. If next BP severe, can give 20mg PO
Nitroprusside: 0.20-4mcg.kg.min IV drip, titrate to effect. Only in critical illness
Nicardipine: 2.5mg/h IV titrating, do not exceed 15mg/h
DO NOT USE: ACEI or ARB
Oral treatment
Labetalol: 100-800mg PO BID-TID (Max dose 2400mg/24hr)
Methyldopa: 250 mg PO BID (Max dose 3g/24hr)
Nifedipine XR: 30-90 mg PO daily (Max dose 120mg/24h)
Pre-Eclampsia with severe features or chronic HTN with superimposed pre-Eclampsia with severe features
Magnesium sulfate for seizure prevention: Given during stabilization prior to expectant management, during delivery, and 24h postpartum. Bolus 4-6g IV with maintenance of 1-2g/h for seizure prevention, titrate and consider no bolus if pt has renal failure. Monitor closely for pulm edema as MgSo4 is a smooth muscle relaxer
Timing for delivery:
Chronic HTN: No earlier than 38w if well controlled
Gestation HTN: 37weeks
Pre-Eclampsia
- Without severe feature: 37 weeks or >34 weeks if IUGR
- With severe feature: at 34 week if severe HTN is only feature. Otherwise deliver after 48hr of steroid if other severe feature present
Chronic HTN with superimposed preeclampsia: at 37 week if no severe features. Otherwise same as preeclampsia with severe feature
Pocket Obstetric and Gynecology by K Joseph Hurt, 2nd edition
Vaginal birth after Cesarean
Appropriate candidates
Hx 1-2 C-section via low transverse hysterotomy.
Inappropriate candidates
Previous classical or T-incision, prior uterine rupture, extensive transfundal uterine surgery (ex: myomectomy), and patient with any contraindication to vaginal delivery.
Online NICHD VBAC success rate calculator
Delivery Considerations
- Misoprostol should NOT be used for TOLAC induction given elevated risk of uterine rupture
- Continuous fetal monitoring should be employed
- Maintain high suspicion for signs/sx of uterine rupture, including new onset uterine pain, loss of fetal station, new fetal heart race tracing abnormalities (most common), vaginal bleeding and maternal hemodynamic instability
- Staff (OB and anesthesia) must be immediately available for emergent c-section
Pocket Obstetrics and gynecology by K Joeph Hurt 2nd edition
Post Dates Management
- Review gestational dating
- AFI/BPP and NST at 41 weeks and repeat once to twice a week
- Consider membrane stripping at 39 weeks
- Consider induction at 41 weeks and cervical ripening agents
Gestational Diabetes
Universal screening start at 24-248 weeks.
Consider screening earlier in all women with BMI >25 and one or more risk factors:
- Physical inactivity
- 1st degree relative with DM
- High-risk ethnicity (AA, Latino, NA, Asian, Pacific Islander)
- Previous GDM or previous more than equal to 4000g birth
- Hypertension
- PCOS
- Prepregnancy BMI >40
Screening test:
1hr OGTT (50g): serum >130-140 , Positive screening test -->3hr OGTT (100g)
3hr OGTT (100g): Fasting plus 1hr, 2hr, 3hr. 2 or more abnormal values = GDM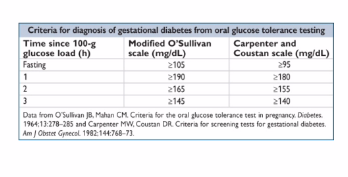
Management
- Nutrition advise, diet/exercise and 4x/day blood glucose testing (fasting + 2hr postprandial). Goals for fasting 60-90 ; 2hr post prandial : <120
- If inadequate control --> insulin (NPH q12h with preprandial short acting insulin 3-4 x daily) 0.7-2u/kg current patient weight . Oral agents used much less these days (glyburide and metformin)
- Insulin management: with active labor or gluc <70mg/dL start D5NS IVF, check fingerstick glucose qhourly. Usually pregestational DM --> IV insulin drip and titrate
- NST once or twice weekly starting at 32 weeks for controlled on medication without severe feature
- NST twice weekly starting at 32 weeks for poorly controlled
- Delivery 39-40w unless poorly controlled
- Consider C-sec for EFW >4500g
- GDM resolves with delivery so do post partum 75g glucose (2h OGTT) at 6 weeks post partum to identify non-gestational DM for all GDM patients
Pocket Obstetrics and gynecology by K Joeph Hurt 2nd edition
Twins
At risk for hyperemesis, GDM, HTN, hemorrhage, cesaeran, postpartum depression, preeclampsia, preterm delivery, IUGR, birth/genetic defects
- Pre-term labor education
- Fetal kick count starting at 28 weeks (10 kicks/movement within 2hrs or less)
- NST weekly starting at 36 weeks for uncomplicated dichorionic
- NST weekly starting at 32 weeks for uncomplicated monochorionic diamniotic.
Management
- Dichorionic twins
- Early US for chorionicity, detailed US at 18-22 wks, growth every 4-6 weeks, delivery at 38 weeks
- Monochorionic diamniotic twin
- Early US for chorionicity, US for TTTS (twin to twin transfusion syndrome) f/u every 2 weeks at 16 weeks, growth every 4 weeks, delivery at 34-37 weeks
- Consults with perinatologist for discordant growth, monoamniotic twins (cord accidents) or monochorionic twins (twin to twin transfusions)
Pocket Obstetrics and gynecology by K Joeph Hurt 2nd edition
ER precautions in Term Pregnancy
- Regular painful contraction every 5 minutes (nulliparous) or every 10 minutes (multiparous), or sooner if long distance to hospital or history of precipitous delivery
- Rupture of membrane
- Vaginal bleeding
- No or decreased fetal movement (<10 kicks in 2hrs)
Medication in Obstetrics
Minimize all medication use during pregnancy (especially in 1st TM), unless clearly indicated!
FDA pregnancy categories
A: No risk in controlled human studies
B: No risk in controlled animal studies and no risk seen in humans
C: Small risk in controlled animal studies, but not seen or not studied in humans
D: Strong evidence of risk in humans but benefit may outweigh tisk
X: High risk - never to be used in pregnant humans
Analgesics
- Acetaminophen - B / compatible with breastfeeding
- Ibuprofen - C 1st/2ndTM ; D 3rdTM / compatible with breastfeeding
- Fentanyl - C / compatible with breast feeding
- Hydromorphone (Dilaudid) - C / compatible with breast feeding
- Morphine - C / Compatible with breast feeding
- Oxycodone (Percoset) - B / Compatible with breast feeding
- Hydrococone (Vicodin) - C / Compatible with breast feeding
Antibiotics
- Ampicillin - B / Compatible with breast feeding
- Amoxicillin - B / Compatible with breast feeding
- Cefazolin - B / Compatible with breast feeding
- Gentamicin - D / Compatible with breast feeding
- Clindamycin - B / Avoid if possible in breast feeding, monitor infant
- Cipro - C (avoid in pregnancy) / Avoid if possible in breast feeing, monitor infant
- TMP-SMX - D / infant risk minimal in breast feeding
- Nitrofurantoin - B in 1st and 2nd TM ; D in 3rd TM / Compatible with breast feeding
- Ceftriaxone - B / Compatible with breast feeding
- Zosyn - B / Compatible with breast feeding
- Erythromycin - B / infant risk minimal in breast feeding
- Vanco - C / infant risk cannot be ruled out in breast feeding
- Keflex - B / Compatible with breast feeding
- Flagyl - B / Infant risk cannot be ruled out, avoid if possible in breast feeding
- Doxycycline - D / avoid in breast feeding
Anticoagulation
- Lovenox - B / Compatible with breast feeding
- Heparin - C / Compatible with breast feeding
- Warfarin - X / Compatible with breast feeding
Antiemetics
- Vitamin B6 - A / Compatible with breast feeding
- Doxylamine - C / May decrease breastmilk supply
- Prochlorperazine - C / Infant risk cannot be ruled out in breast feeding
- Metoclopromide - B / Infant risk cannot be ruled out in breast feeding
- Ondansetron - B / Infant risk cannot be ruled out in breast feeding
- Promethazine HCl - C / Compatible with breast feeding
Diabetes medication
- Metformin - B / Compatible with breast feeding
- Sulfonylurea - B / infant risk cannot be ruled out
- Insulin - B / Compatible with breast feeding
Hypertension or preeclampsia treatment
- Hydralazine - C / Compatible with breast feeding
- Labetalol - C / Compatible with breast feeding
- Magnesium sulfate - A / Compatible with breast feeding
- Nifedipine - C / Compatible with breast feeding
Psychiatric / substance abuse medications
- Zolpidem - C / Caution with breastfeeding
- Buproprion - C / Compatible with breast feeding
- Citalopram, fluoxetine, Sertraline - C / Compatible with breast feeding
- Trazodone - C / Compatible with breast feeding
- Lorazepam - D / Compatible with breast feeding
https://www.aafp.org/afp/2003/0615/p2517.html
Pocket Obstetric and Gynecology by K Joseph Hurt, 2nd edition
PAP Smear Referral Guideline
Algorithm 2013 Univ Washington
PEDS
Peds Inpatient Expectation
- You will receive an email from valley children for the on-boarding package. Part of this package, you need to have also go to our employee health to get mask fitting because VCH using a different mask than the one we have at SAMC.
- On your first day, you will meet at the GME office. To get to GME office, go through the main entrance and turn left at the security desk. The GME office will be on your right side. (you can also ask the security and he/she will direct you). First day will start at 8am for orientation then they will drop you off to the inpatient team you are assigned to.
- In general your shift is from 6.30AM to 5PM. Sign out start at 6.30 in Nielsen room but you may want to consider to come earlier if you need longer time to see for your patients since you likely will be getting new patients everyday from the night admission.
- Each morning your senior will assign your patients. Your senior will contact the attending regarding the time of rounding but usually starting between 8.30 to 9AM.
- They are rounding using family centered round and presenting using system based not problem based. Everything will be explained during your rotation
- There will also be a morning report T/W/Th from 7.30 to 8AM
- They provide burrito breakfast that you can get from the GME lounge
- Didactic protected time at VCH is on Wedneday at noon. Lunch also provided
- To see your schedule can go to amion.com --> secure login --> Pass: VCMG@9300 res
*note the space between the “0” and “r”
Developmental Milestones
Newborn
- Has periods of wakefulness; looks at parent's eyes when being held
- Calms when picked up
Verbal Language:
- Communicates discomfort through crying and behaviors such as facial expressions, body movements
- Moves or calms to parent's voice
Gross Motor:
- Moves in response to visual or auditory stimuli
- Reflexively moves arms and legs, observed in the moro reflex
Fine Motor:
- Keeps hands in fist
- Automatically grasps others' fingers or objects
1 month
- Looks at parents
- Has self-comforting behaviors such as bringing hands to mouth
- Become fussy when bored and calms when picked up or spoken to
- Looks briefly at objects
Verbal Language:
- Alerts to unexpected sounds
- Turns to parent's voice
- Has different types of cries for hunger, tiredness
Gross Motor:
- Moves both arms and both legs together
- Holds chin up when on stomach
Fine Motor:
- Opens fingers slightly when at rest
2 months
- Calms down when spoken to or picked up
- Looks at your face
- Seems happy to see you when you walk up to her
- Smiles when you talk to or smile at her
Language/Communication Milestones
- Makes sounds other than crying
- Reacts to loud sounds
Cognitive Milestones
- Watches you as you move
- Looks at a toy for several seconds
Movement/Physical Development Milestones
- Holds head up when on tummy
- Moves both arms and both legs
- Opens hands briefly
4 months
- Smiles on his own to get your attention
- Chuckles (not yet a full laugh) when you try to make her laugh
- Looks at you, moves, or makes sounds to get or keep your attention
Language/Communication Milestones
- Makes sounds like “oooo”, “aahh” (cooing)
- Makes sounds back when you talk to him
- Turns head towards the sound of your voice
Cognitive Milestones
- If hungry, opens mouth when she sees breast or bottle
- Looks at his hands with interest
Movement/Physical Development Milestones
- Holds head steady without support when you are holding her
- Holds a toy when you put it in his hand
- Uses her arm to swing at toys
- Brings hands to mouth
- Pushes up onto elbows/forearms when on tummy
6 months
- Knows familiar people
- Likes to look at self in a mirror
- Laughs
Language/Communication Milestones
- Takes turns making sounds with you
- Blows “raspberries” (sticks tongue out and blows)
- Makes squealing noises
Cognitive Milestones
- Puts things in her mouth to explore them
- Reaches to grab a toy he wants
- Closes lips to show she doesn’t want more food
Movement/Physical Development Milestones
- Rolls from tummy to back
- Pushes up with straight arms when on tummy
- Leans on hands to support himself when sitting
9 months
- Is shy, clingy, or fearful around strangers
- Shows several facial expressions, like happy, sad, angry, and surprised
- Looks when you call her name
- Reacts when you leave (looks, reaches for you, or cries)
- Smiles or laughs when you play peek-a-boo
Language/Communication Milestones
- Makes a lot of different sounds like “mamamama” and “bababababa”
- Lifts arms up to be picked up
Cognitive Milestones
- Looks for objects when dropped out of sight (like his spoon or toy)
- Bangs two things together
Movement/Physical Development Milestones
- Gets to a sitting position by herself
- Moves things from one hand to her other hand
- Uses fingers to “rake” food towards himself
- Sits without support
12 months
- Plays games with you, like pat-a-cake
Language/Communication Milestones
- Waves “bye-bye”
- Calls a parent “mama” or “dada” or another special name
- Understands “no” (pauses briefly or stops when you say it)
Cognitive Milestones
- Puts something in a container, like a block in a cup
- Looks for things he sees you hide, like a toy under a blanket
Movement/Physical Development Milestones
- Pulls up to stand
- Walks, holding on to furniture
- Drinks from a cup without a lid, as you hold it
- Picks things up between thumb and pointer finger, like small bits of food
15 months
- Copies other children while playing, like taking toys out of a container when another child does
- Shows you an object she likes
- Claps when excited
- Hugs stuffed doll or other toy
- Shows you affection (hugs, cuddles, or kisses you)
Language/Communication Milestones
- Tries to say one or two words besides “mama” or “dada,” like “ba” for ball or “da” for dog
- Looks at a familiar object when you name it
- Follows directions given with both a gesture and words. For example, he gives you a toy when you hold out your hand and say, “Give me the toy.”
- Points to ask for something or to get help
Cognitive Milestones
- Tries to use things the right way, like a phone, cup, or book
- Stacks at least two small objects, like blocks
Movement/Physical Development Milestones
- Takes a few steps on his own
- Uses fingers to feed herself some food
18 months
- Moves away from you, but looks to make sure you are close by
- Points to show you something interesting
- Puts hands out for you to wash them
- Looks at a few pages in a book with you
- Helps you dress him by pushing arm through sleeve or lifting up foot
Language/Communication Milestones
- Tries to say three or more words besides “mama” or “dada”
- Follows one-step directions without any gestures, like giving you the toy when you say, “Give it to me.”
Cognitive Milestones
- Copies you doing chores, like sweeping with a broom
- Plays with toys in a simple way, like pushing a toy car
Movement/Physical Development Milestones
- Walks without holding on to anyone or anything
- Scribbles
- Drinks from a cup without a lid and may spill sometimes
- Feeds herself with her fingers
- Tries to use a spoon
- Climbs on and off a couch or chair without help
24 months
- Notices when others are hurt or upset, like pausing or looking sad when someone is crying
- Looks at your face to see how to react in a new situation
Language/Communication Milestones
- Points to things in a book when you ask, like “Where is the bear?”
- Says at least two words together, like “More milk.”
- Points to at least two body parts when you ask him to show you
- Uses more gestures than just waving and pointing, like blowing a kiss or nodding yes
Cognitive Milestones
- Holds something in one hand while using the other hand; for example, holding a container and taking the lid off
- Tries to use switches, knobs, or buttons on a toy
- Plays with more than one toy at the same time, like putting toy food on a toy plate
Movement/Physical Development Milestones
- Kicks a ball
- Runs
- Walks (not climbs) up a few stairs with or without help
- Eats with a spoon
30 months
- Plays next to other children and sometimes plays with them
- Shows you what she can do by saying, “Look at me!”
- Follows simple routines when told, like helping to pick up toys when you say, “It’s clean-up time.”
Language/Communication Milestones
- Says about 50 words
- Says two or more words, with one action word, like “Doggie run”
- Names things in a book when you point and ask, “What is this?”
- Says words like “I,” “me,” or “we”
Cognitive Milestones
- Uses things to pretend, like feeding a block to a doll as if it were food
- Shows simple problem-solving skills, like standing on a small stool to reach something
- Follows two-step instructions like “Put the toy down and close the door.”
- Shows he knows at least one color, like pointing to a red crayon when you ask, “Which one is red?”
Movement/Physical Development Milestones
- Uses hands to twist things, like turning doorknobs or unscrewing lids
- Takes some clothes off by himself, like loose pants or an open jacket
- Jumps off the ground with both feet
- Turns book pages, one at a time, when you read to her
3 years
- Calms down within 10 minutes after you leave her, like at a childcare drop off
- Notices other children and joins them to play
Language/Communication Milestones
- Talks with you in conversation using at least two back-and-forth exchanges
- Asks “who,” “what,” “where,” or “why” questions, like “Where is mommy/daddy?”
- Says what action is happening in a picture or book when asked, like “running,” “eating,” or “playing”
- Says first name, when asked
- Talks well enough for others to understand, most of the time
Cognitive Milestones
- Draws a circle, when you show him how
- Avoids touching hot objects, like a stove, when you warn her
Movement/Physical Development Milestones
- Strings items together, like large beads or macaroni
- Puts on some clothes by himself, like loose pants or a jacket
- Uses a fork
4 years
- Pretends to be something else during play (teacher, superhero, dog)
- Asks to go play with children if none are around, like “Can I play with Alex?”
- Comforts others who are hurt or sad, like hugging a crying friend
- Avoids danger, like not jumping from tall heights at the playground
- Likes to be a “helper”
- Changes behavior based on where she is (place of worship, library, playground)
Language/Communication Milestones
- Says sentences with four or more words
- Says some words from a song, story, or nursery rhyme
- Talks about at least one thing that happened during his day, like “I played soccer.”
- Answers simple questions like “What is a coat for?” or “What is a crayon for?”
Cognitive Milestones
- Names a few colors of items
- Tells what comes next in a well-known story
- Draws a person with three or more body parts
Movement/Physical Development Milestones
- Catches a large ball most of the time
- Serves himself food or pours water, with adult supervision
- Unbuttons some buttons
- Holds crayon or pencil between fingers and thumb (not a fist)
5 years
- Follows rules or takes turns when playing games with other children
- Sings, dances, or acts for you
- Does simple chores at home, like matching socks or clearing the table after eating
Language/Communication Milestones
- Tells a story she heard or made up with at least two events. For example, a cat was stuck in a tree and a firefighter saved it
- Answers simple questions about a book or story after you read or tell it to him
- Keeps a conversation going with more than three back-and-forth exchanges
- Uses or recognizes simple rhymes (bat-cat, ball-tall)
Cognitive Milestones
- Counts to 10
- Names some numbers between 1 and 5 when you point to them
- Uses words about time, like “yesterday,” “tomorrow,” “morning,” or “night”
- Pays attention for 5 to 10 minutes during activities. For example, during story time or making arts and crafts (screen time does not count)
- Writes some letters in her name
- Names some letters when you point to them
Movement/Physical Development Milestones
CDC’s Developmental Milestones
Immunization Schedule
Peds Immunization
Can also download cdc vaccination schedule app via your phone store
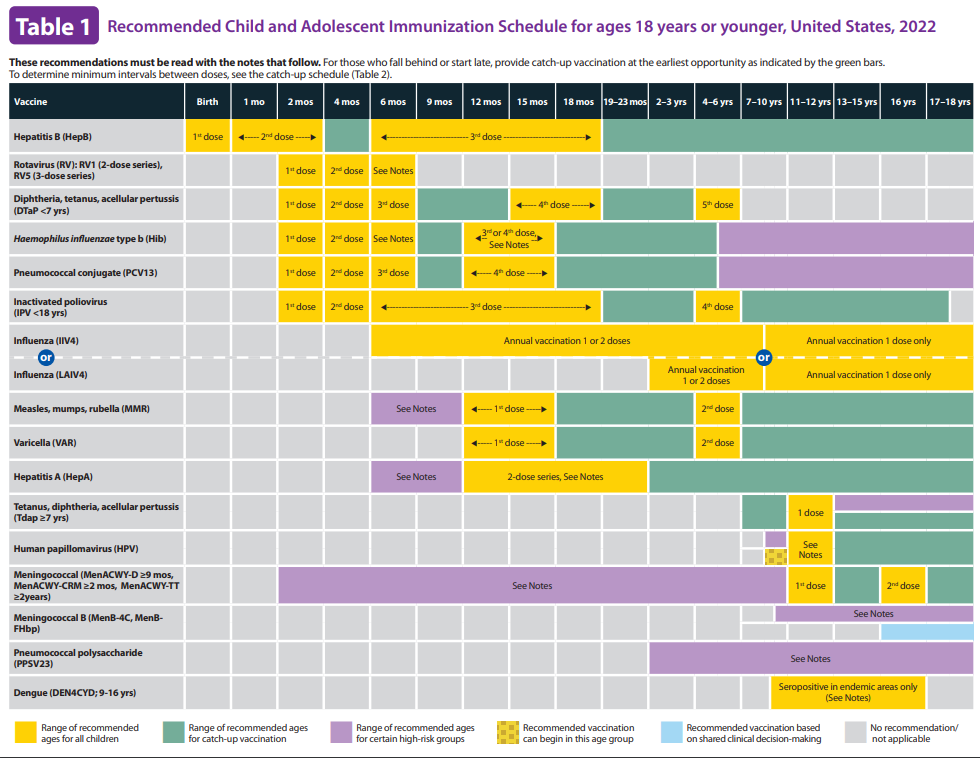
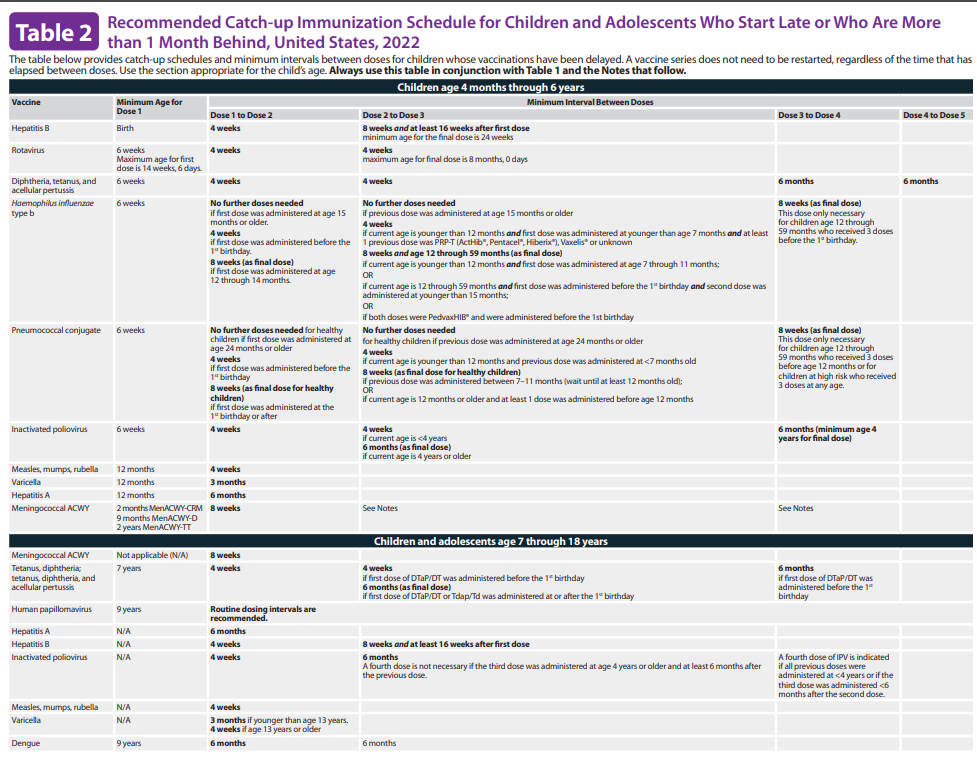
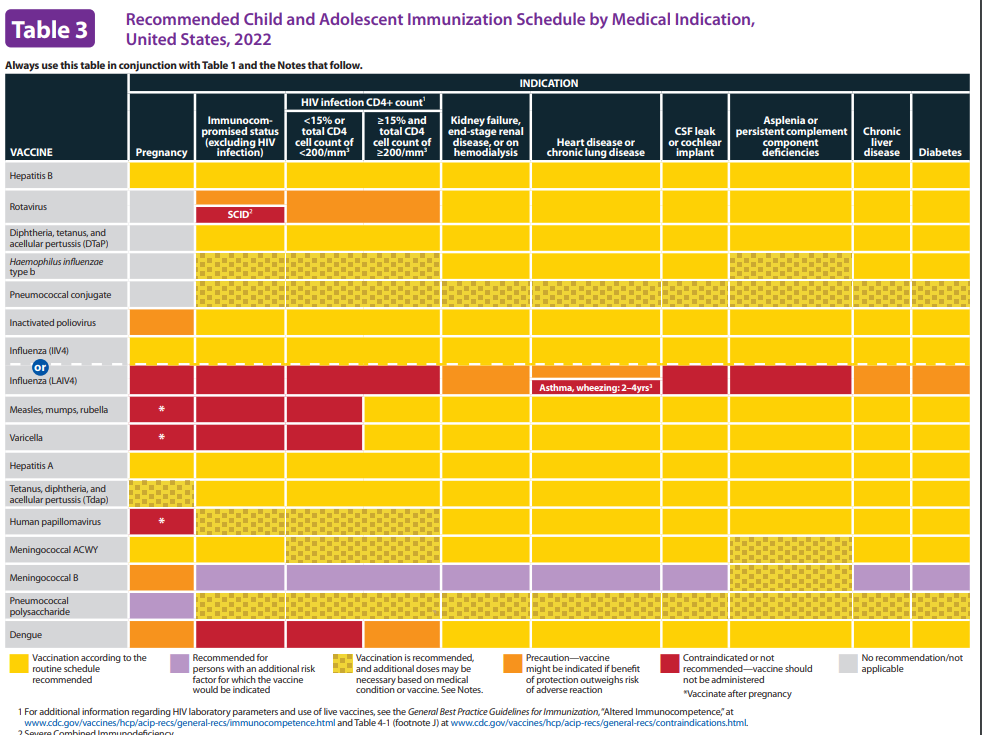
Child and Adolescents Immunization
Adult Immunization
Download CDC vaccination schedule via your phone app
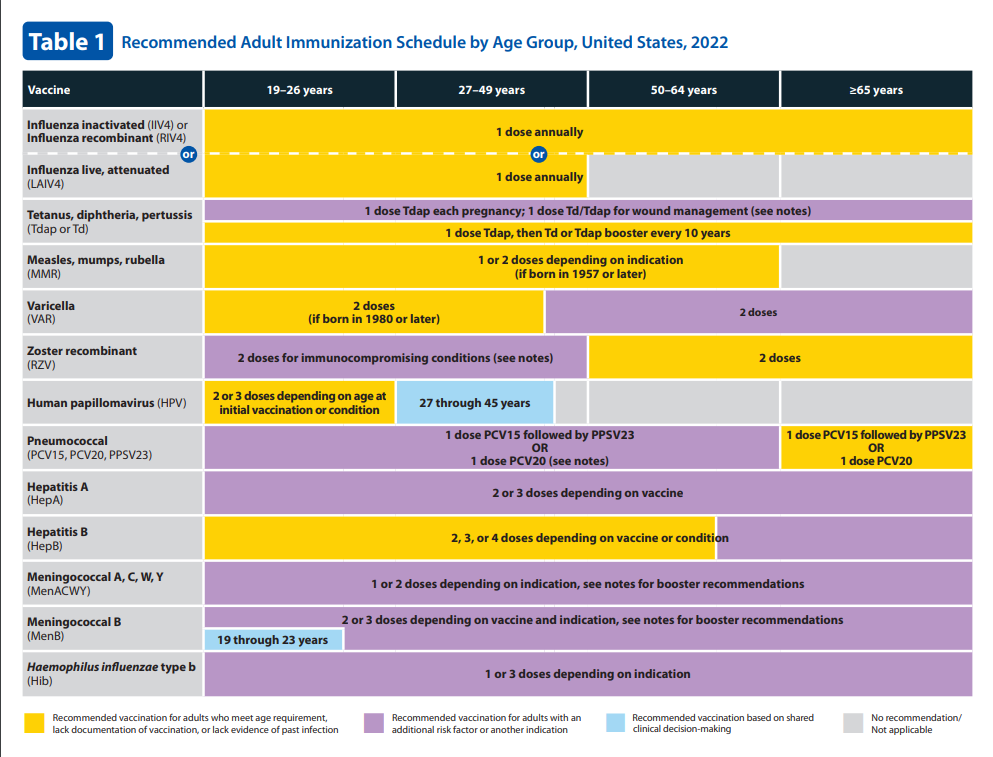
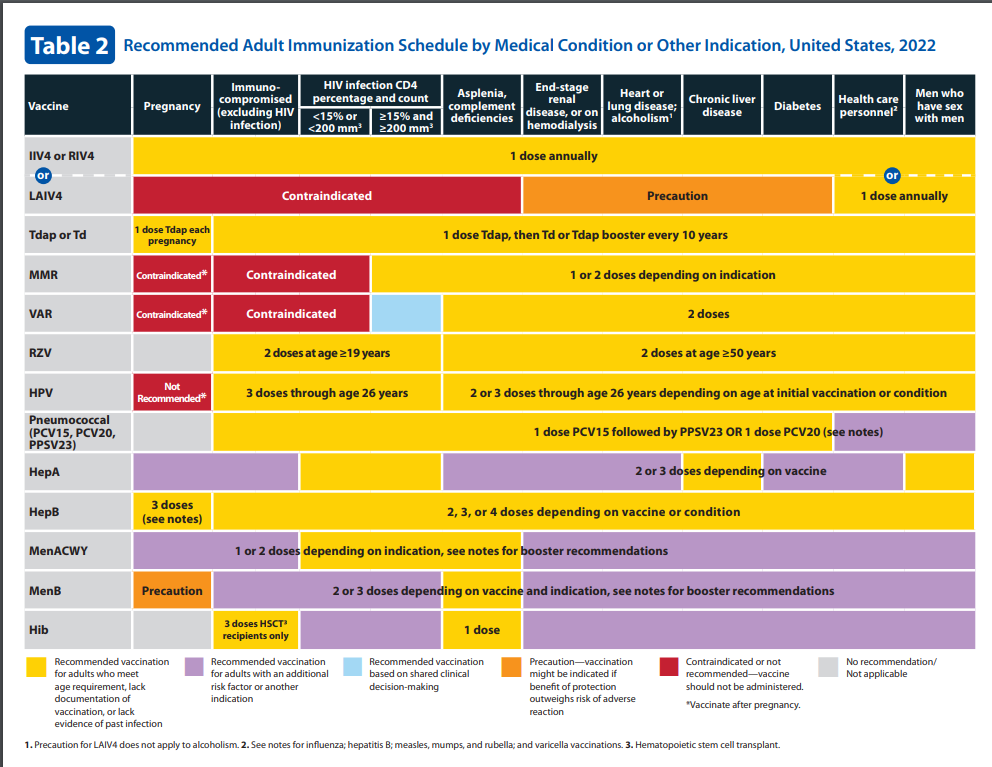
ACLS Protocols
VFib/Pulseless VT/Asystole/PEA
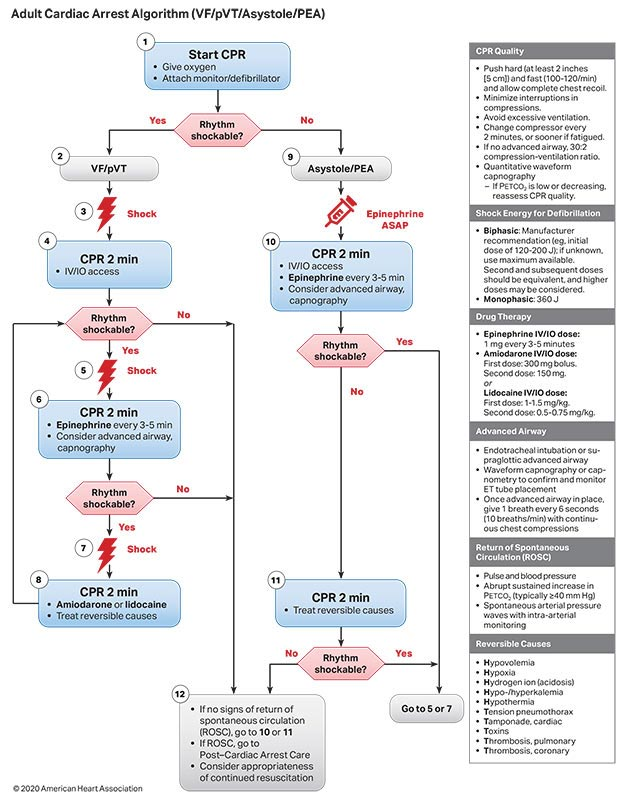
Bradycardia
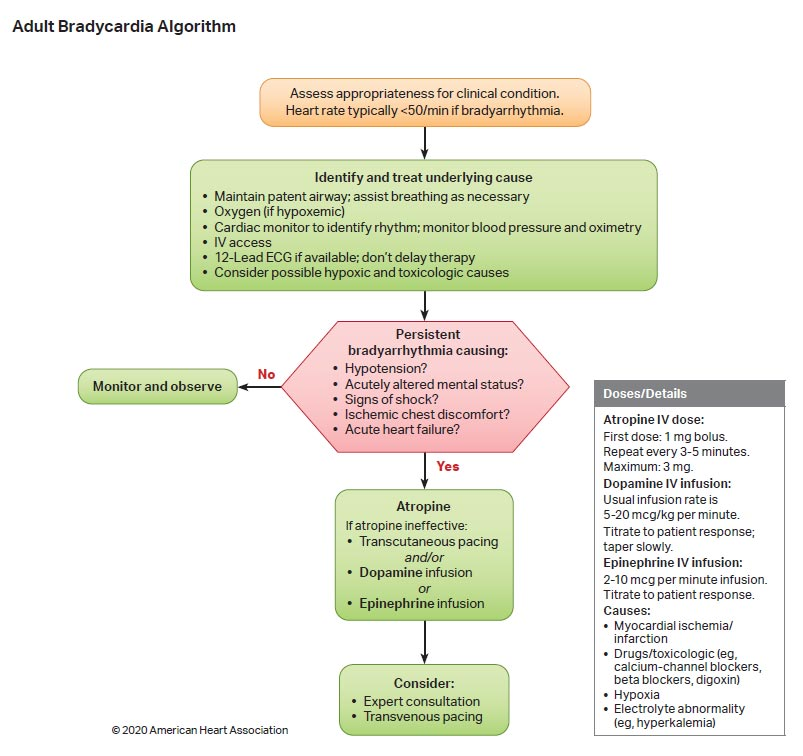
Tachycardia
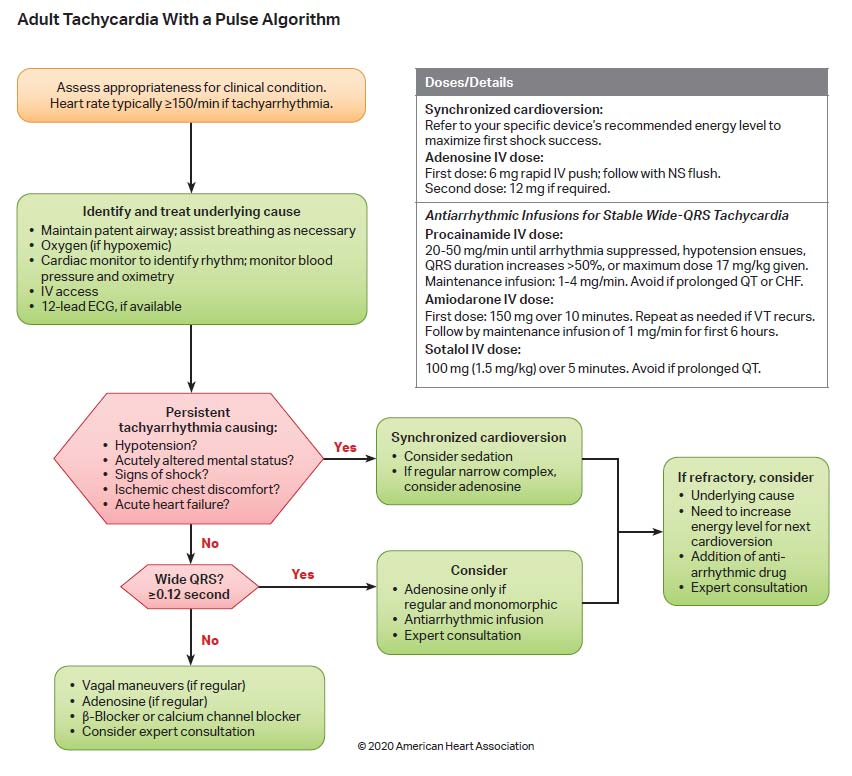
Outpatient Service
Expectations
-
Outpatient Preceptorship
-
Precept all patients with attending
-
-
All Residents should:
-
When on AMB rotation, do NOT wear scrubs.
-
Prepare prior to seeing patient (look at chief complaint, any relevant hospitalizations, consults, history, new medications, studies, etc...)
-
Prior to presenting: form an A&P to present and research any relevant diagnostics and treatments. If unsure, ok to ask but have an informed question
-
Include differentials, explain supportive evidence for one or the other
-
Ex: Express the most likely diagnosis, then the next possible dx, and why it is or isn't likely to be a dangerous diagnosis
-
-
Be specific. If ordering medications, vaccinations, or tests - name them and their dose
-
Do NOT sign orders until you have precepted with the attending and the attending has had a chance to review them
-
Be mindful of patients waiting in the exam room
-
Must complete Billing (see Billing Section)
-
Document and consent for all procedures
-
Use Athena Capture for all Derm cases
-
Must use Chaperon (MA) for sensitive exams
-
Must use Language Line if translation is needed
-
Conduct Video Visits in the Exam Room using Cliq or Doximity
-
Be mindful of HIPPA when discussing patients outside of the exam room
-
All vaccines must be placed as an order first prior to Athena Text or verbal orders to MAs
-
You have 24hrs to submit all chart notes to be signed off by your preceptor attending unless there's a valid excuse
Morning Report
Mon and Tue from 8-8:30AM
Location: NW Clinic Back Conference Room
Mon
Board Review Questions
Tue
-
Stanford Clinical Skills
-
Patient Cases
Attendance will be taken during your AMB rotation
Stanford Diabetes ECHO
GME SAMC IM and FP have signed a collaborative agreement with Stanford University's Diabetes ECHO project providing the latest guidelines and management of Type 1 and 2 Diabetes.
All Residents on AMB rotation are expected to attend the Zoom conference on Thur 12:15-1:15 PM as posted in the Didactics Calendar. Lecture topics and Case presentation will be given.
Case presentation if requested by Stanford will be assigned or voluntarily chosen. Any resident who presents a patient case will be given Scholarly Activity credit
Attendance will be taken, please use Stanford's Zoom Chat box with your [name], St. Agnes Medical Center
Screening Schedule
USPSTF screening
Abdominal Aortic Aneurysm: Screening:
- The USPSTF recommends 1-time screening for abdominal aortic aneurysm (AAA) with ultrasonography in men aged 65 to 75 years who have ever smoked.
Asymptomatic Bacteriuria in Adults: Screening: pregnant persons
- The USPSTF recommends screening for asymptomatic bacteriuria using urine culture in pregnant persons.
Breast Cancer: Screening: women aged 50 to 74 years
- The USPSTF recommends biennial screening mammography for women aged 50 to 74 years.
Cervical Cancer: Screening: women aged 21 to 65 years
- The USPSTF recommends screening for cervical cancer every 3 years with cervical cytology alone in women aged 21 to 29 years. For women aged 30 to 65 years, the USPSTF recommends screening every 3 years with cervical cytology alone, every 5 years with high-risk human papillomavirus (hrHPV) testing alone, or every 5 years with hrHPV testing in combination with cytology (cotesting).
Chlamydia and Gonorrhea: Screening: sexually active women, including pregnant persons
- The USPSTF recommends screening for chlamydia in all sexually active women 24 years or younger and in women 25 years or older who are at increased risk for infection.
- The USPSTF recommends screening for colorectal cancer in adults aged 45 to 75 years.
- The USPSTF recommends screening for depression in the general adult population, including pregnant and postpartum women.
- The USPSTF recommends screening for major depressive disorder (MDD) in adolescents aged 12 to 18 years.
Gestational Diabetes: Screening:
- The USPSTF recommends screening for gestational diabetes in asymptomatic pregnant persons at 24 weeks of gestation or after.
Hepatitis B Virus Infection in Adolescents and Adults:
- The USPSTF recommends screening for hepatitis B virus (HBV) infection in adolescents and adults at increased risk for infection.
- The USPSTF recommends screening for hepatitis B virus (HBV) infection in pregnant women at their first prenatal visit
Hepatitis C Virus Infection in Adolescents and Adults
- The USPSTF recommends screening for hepatitis C virus (HCV) infection in adults aged 18 to 79 years.
Human Immunodeficiency Virus (HIV) Infection:
- The USPSTF recommends that clinicians screen for HIV infection in adolescents and adults aged 15 to 65 years.
- The USPSTF recommends that clinicians screen for HIV infection in all pregnant persons, including those who present in labor or at delivery whose HIV status is unknown.
Hypertension in Adults: Screening: adults 18 years or older without known hypertension
- The USPSTF recommends screening for hypertension in adults 18 years or older with office blood pressure measurement (OBPM).
- The USPSTF recommends that clinicians screen for intimate partner violence (IPV) in women of reproductive age and provide or refer women who screen positive to ongoing support services.
- The USPSTF recommends annual screening for lung cancer with low-dose computed tomography (LDCT) in adults aged 50 to 80 years who have a 20 pack-year smoking history and currently smoke or have quit within the past 15 years. Screening should be discontinued once a person has not smoked for 15 years or develops a health problem that substantially limits life expectancy or the ability or willingness to have curative lung surgery.
Osteoporosis to Prevent Fractures: Screening: women 65 years and older
- The USPSTF recommends screening for osteoporosis with bone measurement testing to prevent osteoporotic fractures in women 65 years and older.
Prediabetes and Type 2 Diabetes:
- The USPSTF recommends screening for prediabetes and type 2 diabetes in adults aged 35 to 70 years who have overweight or obesity.