Algorithm For Acid Base Disorders
Before You Begin: Gather Data
What lab tests do you need?
- ABG vs. VBG
- VBG can provide reliable estimation for pH (0.02-0.04 lower than ABG) and HCO3 (1-2 mEq higher than ABG).
- pCO2 on VBG is higher than arterial PaO2 by 4-9mmHg.
- ABG is necessary to accurately assess PaCO2 in hypercapnia or severe shock.
- BMP.
- Albumin.
Step 1: Determine Primary Acid-Base Disturbance.
- Remember that chronic acid-base disturbance(s) and/or mixed acute acid-base disturbances can be obscured by a normal pH.
- Consider the following “normal” values:
• Arterial pH: 7.40
• Arterial pCO2: 40
• Bicarb (HCO3): 24
• Anion gap: 12 - Acidemia
• pH < 7.38
• Primary disturbance
• Respiratory acidosis = pCO2 > 42
• Metabolic acidosis = HCO3 < 22 - Alkalemia
• pH > 7.42
• Primary disturbance
• Respiratory alkalosis = pCO2 < 38
• Metabolic alkalosis = HCO3 > 26
Step 2a: Calculate and Interpret the Anion Gap
- Anion gap (AG) = [Na] – [Cl] – [HCO3].
- Normal AG = 8-12 mEq/L with a serum albumin of 4g/dl.
- The normal AG depends on serum albumin. The expected "normal" range for AG can be calculated by 2.5 x albumin (g/dl) +/- 2.
- For severe hypoalbuminemia (2.0 g/dl), the expected gap would be 5 +/- 2, and an AG of 8-12 would be abnormally elevated.
- Paraproteinemia (especially polyclonal or monoclonal IgG) can lower anion gap due to the abundance of cations added to the system; this should be accounted for when evaluating anion gap since it could obscure a truly elevated AG.
- For calculation, >12 is generally used as the cutoff for a high AG. Because 12 is the upper limit of normal, keep in mind that approach might increase specificity for elevated AG at the cost of sensitivity. Because of person-to-person variation in “normal” AG, it can be useful to review a patient’s previous values of AG to establish a baseline and give context to small, acute changes in AG.
- If the AG is elevated, there is an anion gap metabolic acidosis present. Proceed to step 2b.
- If the AG not elevated, there is not an anion gap metabolic acidosis present. Proceed to step 3.
Step 2b: Calculate and Interpret the Excess Anion Gap
- If there is an anion gap, determine whether the excess in AG fully explains the drop in bicarbonate.
- For every 1 unit increase in AG (△AG↑) from its upper limit of normal value (12), there is an expected 1 drop in HCO3 (△HCO3↓) from its “normal” value (24).
- If the AG and HCO3 are balanced, (△HCO3 ± 5mmol/L ≈ △AG), there is no concurrent metabolic process.
- If the HCO3 is lower than expected (△HCO3 ± 5mmol/L > △AG), there is a concurrent non-elevated anion gap metabolic acidosis as evidenced by a reduction of HCO3.
- If the HCO3 is higher than expected (△HCO3 ± 5mmol/L < △AG), there is a concurrent metabolic alkalosis as evidenced by an excess of HCO3.
- The 5mmol/L correction accounts for the normal range of bicarbonate.
- Alternate approach to answer this question: “correcting” the bicarb.
- Corrected HCO3 = HCO3 + (AG - 12).
- If the sum is greater than the usual bicarbonate range (> 28), there is a concomitant metabolic alkalosis. If the sum is less than the usual bicarbonate range (< 22), there is a concomitant non-elevated anion gap metabolic acidosis.
- Finally, there is a third approach to this same problem, “the delta-delta,” which is not discussed here.
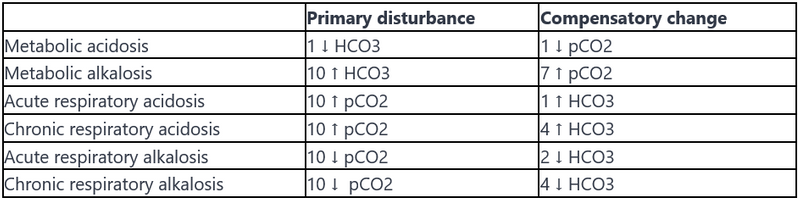
Step 3: Evaluate for Compensation
Evaluate for physiologic compensation for the acid-base disorder.
Any values above or below expected suggest an additional acid-base disturbance; a compensation should not normalize or overcorrect the pH.
The following table gives a quick rule-of-thumb for evaluating compensation. More detailed formulas are listed below.
Common Questions in Metabolic Acidosis
-
What is the pathophysiology of saline-induced normal anion gap (hyperchloremic) metabolic acidosis?The normal anion gap metabolic acidosis resulting from large volume administration of normal saline (NS) can be explained as a dilutional effect on the existing bicarbonate level. This is because NS contains a supraphysiologic concentration of chloride (154 mEq/L) and no bicarbonate; thus it will raise serum chloride while diluting other anions - namely lowering bicarbonate - inducing a metabolic acidosis. This may be avoided by using a balanced intravenous solution such as Lactated Ringer’s or Plasmalyte. These solutions have a lower [Cl-] concentration compared to NS and, most importantly, contain lactate and acetate respectively, which are rapidly metabolized to an equimolar amount of bicarbonate.
-
What are the disadvantages of giving bicarbonate in the setting of acute metabolic acidosis?
-
Can cause an initial transient worsening of intracellular acidosis.
-
Can lead to generation of increased CO2 which causes respiratory acidosis (especially in patients with respiratory failure such as in ARDS).
-
Can represent a large sodium load that can exacerbate hypervolemia.
-
Can worsen hypokalemia.
-
-
The 2008 Surviving Sepsis guidelines recommend against its use in sepsis if pH > 7.15. One can consider temporary NaHCO3 administration in the setting of severe metabolic acidosis (pH < 7.1) or to facilitate permissive hypercarbia. In most cases of normal anion gap metabolic acidosis, it is probably safe. Consider renal replacement therapy in cases of severe acidosis refractory to medical therapy.
Key Points
- It is important to follow a systematic approach each time interpreting a blood gas. Establish the primary disorder. Calculate AG to reveal an anion gap metabolic acidosis (can be hidden when pH is normal but mixed disorders are present). Compare △AG and △HCO3 to look for concurrent metabolic alkalosis or normal anion gap metabolic acidosis. Use a compensation chart/formula to reveal “overcompensation” or “undercompensation” which indicates the presence of another disorder.
- The presence of a normal pH with abnormal pCO2 and bicarbonate suggests a mixed acid-base disorder with counterbalancing acidosis and alkalosis.
- The pCO2 and serum bicarbonate typically move in parallel with an isolated acid-base disorder; both are high OR both are low. For example, a respiratory acidosis will have an increased pCO2 with a compensatory increase in serum bicarbonate. If the pCO2 and serum bicarbonate move in opposite directions (one high and one low), then you should consider the possibility of two simultaneous primary acid-base disorders (i.e., a mixed acid-base disorder).
- A mixed acid-based disorder consists of any combination of at least two disorders: two metabolic disturbances OR one respiratory and one metabolic. Triple acid-base disorders include one respiratory disorder (acidosis or alkalosis) with two metabolic disorders (high gap and normal gap metabolic acidosis OR high gap metabolic acidosis and metabolic alkalosis).
No comments to display
No comments to display