Gestational Diabetes
Universal screening start at 24-248 weeks.
Consider screening earlier in all women with BMI >25 and one or more risk factors:
- Physical inactivity
- 1st degree relative with DM
- High-risk ethnicity (AA, Latino, NA, Asian, Pacific Islander)
- Previous GDM or previous more than equal to 4000g birth
- Hypertension
- PCOS
- Prepregnancy BMI >40
Screening test:
1hr OGTT (50g): serum >130-140 , Positive screening test -->3hr OGTT (100g)
3hr OGTT (100g): Fasting plus 1hr, 2hr, 3hr. 2 or more abnormal values = GDM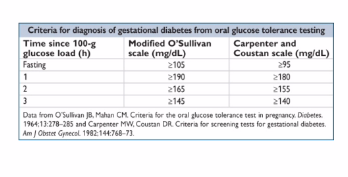
Management
- Nutrition advise, diet/exercise and 4x/day blood glucose testing (fasting + 2hr postprandial). Goals for fasting 60-90 ; 2hr post prandial : <120
- If inadequate control --> insulin (NPH q12h with preprandial short acting insulin 3-4 x daily) 0.7-2u/kg current patient weight . Oral agents used much less these days (glyburide and metformin)
- Insulin management: with active labor or gluc <70mg/dL start D5NS IVF, check fingerstick glucose qhourly. Usually pregestational DM --> IV insulin drip and titrate
- NST once or twice weekly starting at 32 weeks for controlled on medication without severe feature
- NST twice weekly starting at 32 weeks for poorly controlled
- Delivery 39-40w unless poorly controlled
- Consider C-sec for EFW >4500g
- GDM resolves with delivery so do post partum 75g glucose (2h OGTT) at 6 weeks post partum to identify non-gestational DM for all GDM patients
Pocket Obstetrics and gynecology by K Joeph Hurt 2nd edition
No comments to display
No comments to display